You can train a six-year-old. You can train a 96-year-old. The adaptive response to resistance training is the same at both ends. In one of the most-cited trials in geriatrics, ten frail nursing-home residents with a mean age of 90 enrolled in eight weeks of high-intensity resistance training. On average, they gained 174% in quadriceps strength, 9% in mid-thigh muscle size, and a 48% improvement in their walking speed.1 The four-decade-younger version of that response, and everything in between, uses the same adaptive mechanisms. The size of the response and the variability around it shift across the lifespan. The mechanisms producing it do not.7,15
The same prescription drives strength gain across populations: adults and kids, novices and masters lifters, men and women, before and after menopause. The inputs get adjusted for context. This guide walks through what changes in your body when you get stronger, how to make it happen, how to find a program that matches where you are, and what to do when progress stalls.
If you are looking for a strength training guide, you are probably trying to figure out
how to get stronger, what program to follow, how heavy to train, and what to do when progress slows.
This guide explains the main adaptations that drive strength, the training variables that matter most,
and how to choose the right Barbell Medicine program for your goals and training history.
What changes in your body when you get stronger
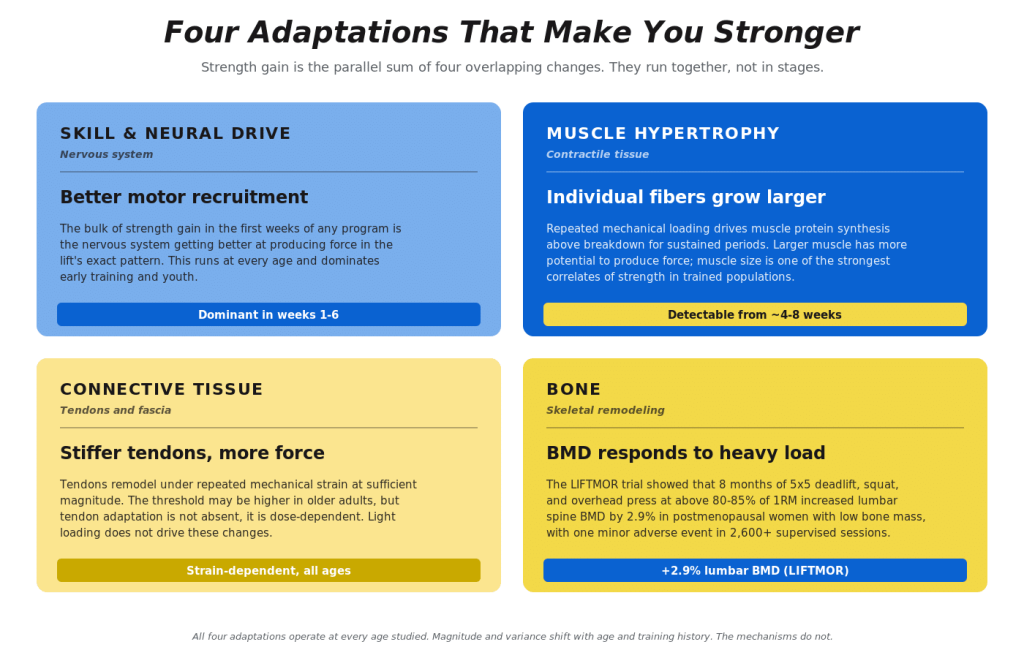
Strength is the amount of force your muscles can produce during a specific task. Improving it requires four overlapping adaptations.
The first is skill and neural drive. Your nervous system gets better at recruiting muscle fibers, coordinating the muscles producing the movement with the muscles opposing it, and producing force in the exact pattern the lift requires. Most of the strength gain in the first weeks of training is skill, not new tissue.3 This is true at every age.
The second is muscle hypertrophy. With repeated loading, muscle protein synthesis exceeds breakdown and individual fibers grow larger. A bigger muscle has more potential to produce force, and muscle size is one of the strongest correlates of strength in trained populations regardless of sex, race, or age.4
The third is connective tissue adaptation. Tendons get stiffer and stronger when they are loaded repeatedly with enough force to deform them. Older tendons need heavier loads to remodel meaningfully, but they still respond. Very light loading does not produce these changes.5
The fourth is bone. Bones get denser and stronger when they’re loaded heavily, particularly when the load runs through the spine. The LIFTMOR trial randomized 101 post-menopausal women with osteopenia or osteoporosis to eight months of supervised heavy resistance and impact training: five sets of five reps at 80-85% of one-rep max in deadlift, back squat, and overhead press, plus jumping chin-ups with drop landings. Compared with low-intensity controls, the LIFTMOR group gained lumbar spine bone mineral density (+2.9% vs -1.2%), knee extensor (quadriceps) strength (+37% vs +5%), back extensor (erector spinae) strength (+36% vs +11%), and improved performance on functional tests like standing up from a chair and walking. One minor adverse event was reported across more than 2,600 supervised sessions.6
All four are running from session one. The size of each contribution shifts with training history and age, but every adaptation is part of the response from the start.
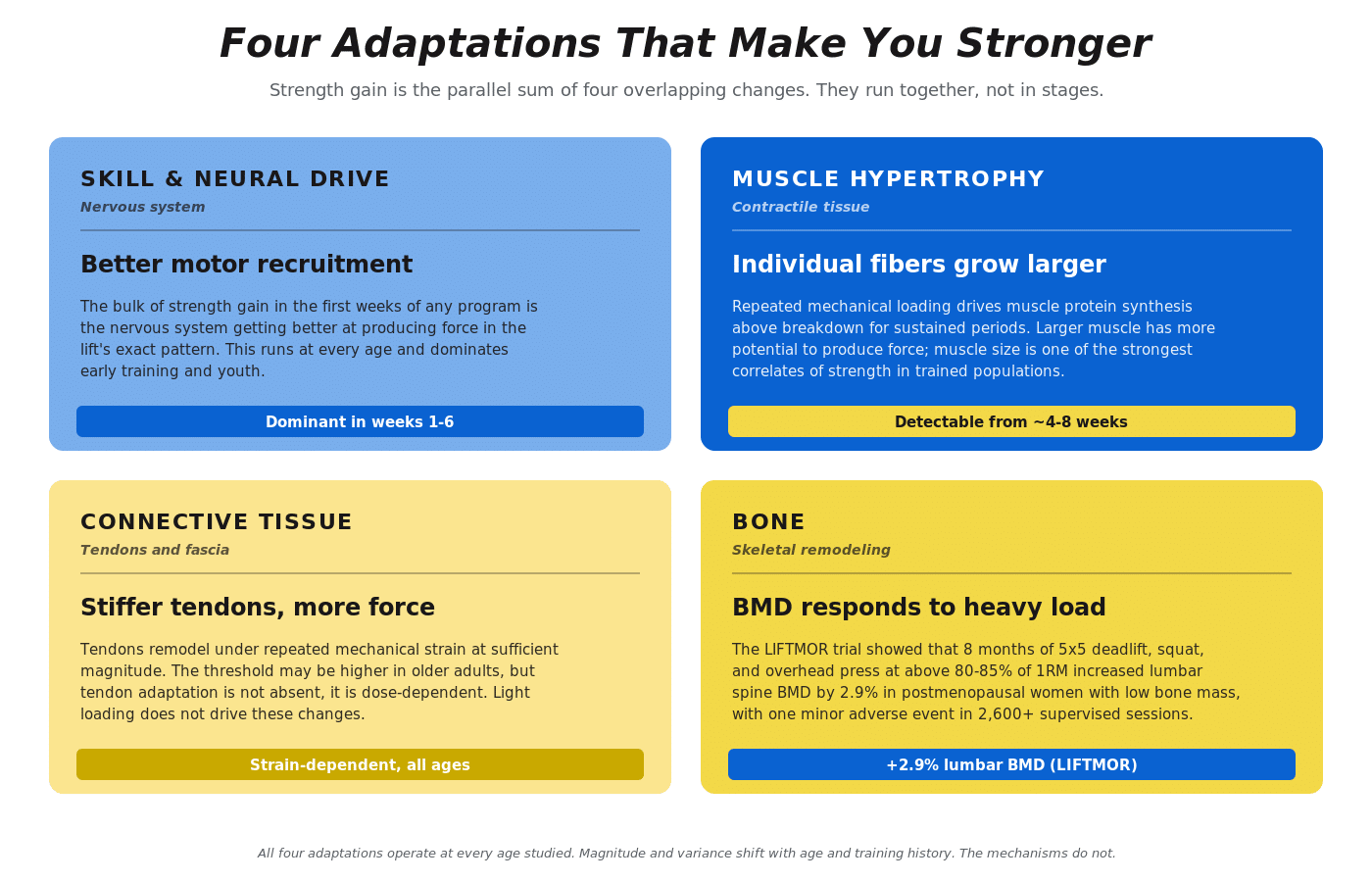
Figure 1. Four adaptations that make you stronger. Skill and neural drive, hypertrophy, connective tissue, and bone all respond to load in parallel; what changes across the lifespan is the absolute magnitude of each, not which mechanisms are operating.
The four inputs that drive those adaptations
Move any of these too far in either direction and the response degrades.
Load. The muscle has to work against meaningful resistance. A meta-analysis of 140 studies found maximal strength gains in untrained adults occurred at around 60% of one-rep max (1RM), and in trained adults around 80% of 1RM.9 Studies in older adults converge on roughly 70 to 79% of 1RM as the productive intensity range, which is also where most adult programs spend the bulk of their work.7 In practice, Rate of Perceived Exertion (RPE) lets you select load by how the set feels, with most strength work landing between RPE 6 and 8. RPE 6 corresponds to four reps in reserve, RPE 8 corresponds to two reps in reserve, and RPE 10 corresponds to no reps in reserve.
Volume. A single set per session is enough to maintain strength in some contexts, but driving meaningful adaptation requires multiple sets. The dose-response shape is roughly logarithmic, meaning more weekly volume produces more growth and strength up to a ceiling that depends on training history and recovery capacity. The evidence here is strong: weekly volume amplifies the effect of both load and effort.8 Most lifters making consistent progress are running between 10 and 20 hard sets per major muscle group per week. Too little produces nothing. Too much accumulates fatigue faster than fitness.
Frequency. Two to four sessions per week is productive for almost everyone. Frequency is mostly an instrument for distributing training across the week; whether you train a muscle group two or four times matters less than whether the weekly total is in a productive range.9
Progression. The training has to match the lifter. As fitness improves, the load has to go up to match. If someone detrains, the load comes back down. The underlying adaptations run on different timescales, and the variance around when they show up is wide, both between people and day to day in the same person. That makes scheduled load increases that ignore whether adaptations have actually occurred a bad bet. Progressive loading can mean adding weight at the same reps and RPE, completing more reps at the same weight and RPE, or completing the same work at a lower RPE and higher bar speed.10 All three count. As Greg Lemond said about cycling, it never gets easier, you just go faster. Same principle in the gym: the effort stays steady, what you can do at that effort goes up.
For a deeper read on how progressive overload actually works in practice, see our three-part series on progressive loading: Part 1, Part 2, and Part 3.
Recovery and nutrition
Adaptation runs continuously between sessions, not just during them. Three environmental inputs determine whether the training you’re doing produces the response you want or just accumulates as stress.
Sleep. Adults who consistently sleep less than about six hours a night perform worse on lifts, recover slower between sessions, and miss training more often.2 Most adults do best with roughly seven to nine hours, with consistent timing. No specific number has been shown to maximize hypertrophy, but chronic short sleep degrades almost every variable that matters for training response.
Protein. For lifters pursuing hypertrophy and strength, target 1.6 to 2.2 g/kg/day, with each meal containing about 0.4 g/kg of protein.11 For general health and maintenance, 1.2 to 1.6 g/kg/day is sufficient. At doses in the productive range, source matters less than total intake. Mixed dietary protein, whey, casein, soy, and pea all work when daily and per-meal targets are met. The per-meal dose matters more in older adults; the apparent “anabolic resistance” of aging shrinks substantially when protein dose and training load are both adequate.12
Energy balance. Strength can be gained, maintained, or lost across a wide range of energy intakes. Modest deficits (roughly 10 to 20% below maintenance) typically allow continued strength gain when protein and training load stay adequate, especially in lifters with body fat to draw from.21 Larger deficits, very low body fat, and inadequate protein can blunt adaptation more aggressively. Maintenance or a slight surplus is the easier setting if hypertrophy is the priority; a deficit is workable if fat loss is the priority and the program is matched accordingly.
Default lifts in BBM programs
If strength is the ability to produce force in a specific task, then any exercise that loads the relevant muscles can drive a training response. Most Barbell Medicine programs default to a small number of compound barbell lifts, where “compound” means the movement crosses multiple joints and trains large amounts of muscle mass at once.
Most of our strength programs default to three barbell lifts: squat, bench press, and deadlift. The reason is partly historical. We came up through powerlifting, those are the three competition lifts, and that’s the programming infrastructure we built around. They aren’t uniquely beneficial movements; they earn their place because they have decades of coaching history behind them, can be loaded heavily, and are easy to track over time. Still, an individual who has different preferences can pick different exercises and do just fine. Similarly, a lifter who cannot squat well due to anatomy, equipment, or injury history can build comparable strength using leg presses, hack squats, split squats, or other variations.
The three barbell lifts that anchor most BBM strength programs are:
Squat. A loaded knee-and-hip flexion under an axial load. Trains the quads, glutes, adductors, and the trunk musculature that resists flexion under the bar. Variations range from low-bar back squat (typical of powerlifting), to high-bar back squat (typical of weightlifting), to front squats, paused squats, tempo squats, and box squats. The choice depends on goals, equipment, and what the lifter can train consistently.
Bench press. A horizontal press performed supine on a bench. Trains the chest, anterior deltoids, and triceps, with stabilization from the upper back and legs. Variations include incline bench, close-grip bench, paused bench, and dumbbell bench. For technique, see the Bench Press Guide.
Deadlift. A loaded hip-hinge lift from the floor. Primarily trains the glutes, hamstrings, adductors, spinal erectors, and grip. Conventional and sumo are the two different stances. Deficit deadlifts, paused deadlifts, and block pulls are common variations.
The press, row, pull-up, and overhead-press patterns fill in the upper-body work. Nearly all of the Barbell Medicine programs allow user-selected exercises for the main lifts, so the program matches the lifter rather than the other way around.
Find your starting point
Where you are in your training history changes how often you can detect a real change in performance, and that determines which program structure is going to feel productive right now. The labels novice, intermediate, advanced describe a detection window: how long it takes to confidently call a real performance change above day-to-day noise. The mechanisms producing the gain are the same throughout.15
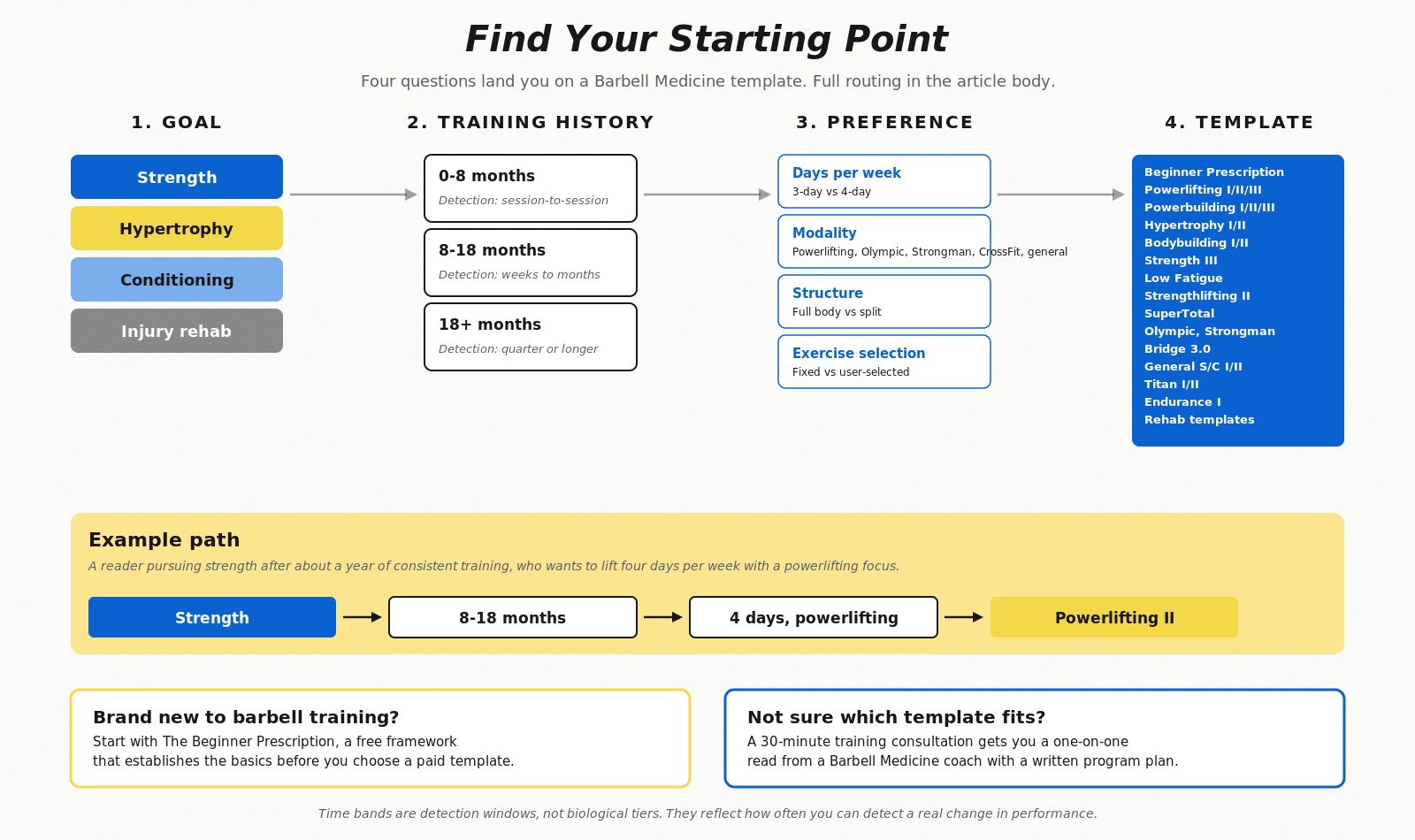
Figure 2. Find your starting point. Goal, training history, and preference route the lifter to a specific Barbell Medicine template. Time bands are detection windows, not biological tiers.
Pick the description that best matches your current situation:
- 0 to 8 months of consistent progressive training. Gains show up week to week and often session to session.
- 8 to 18 months of consistent progressive training. Gains stop showing up session to session and start showing up over weeks.
- 18+ months of consistent progressive training. Progress lives on a longer timescale, often months at a time.
Then pick your primary goal from strength, hypertrophy, conditioning, or injury rehab. See the tables below for our recommendations:
| Goal | 0–8 months | 8–18 months | 18+ months |
| Strength | Strength I | Strength II | Strength IIILow Fatigue |
| Strength + hypertrophy | Powerbuilding I | Powerbuilding IPowerbuilding II | Powerbuilding II |
| Hypertrophy | Hypertrophy I | Hypertrophy IIBodybuilding I | Hypertrophy IIBodybuilding IBodybuilding II |
| Conditioning | General S/C I | General S/C ITitan IEndurance I | General S/C I or IITitan I or IIEndurance I |
| Injury rehab | Knee, Low Back, Shoulder, or Hip Rehab Templates | Same | Same |
If your primary goal is a specific sport, the routing is goal-driven rather than tied to training history. The templates below work across training history bands.
| Sport | Template |
| Olympic weightlifting | Olympic Weightlifting |
| Strongman | Strongman |
| Rowing | Rowing |
| Combined Olympic weightlifting + powerlifting | SuperTotal |
| Olympic + strength with CrossFit-style conditioning | Titan I or II |
If your situation does not fit any of these neatly, a training consultation gets you a one-on-one read from a Barbell Medicine coach.
Find your next program
Choose a strength program that matches your training history
Whether you are newer to lifting or have years of training behind you, Barbell Medicine programs are built around progressive loading, fatigue management, and flexible exercise selection.
How age and sex change the prescription (mostly, they don’t)
Age and sex have smaller effects on the response to training than most people assume. When two lifters match on training history, load, recovery, and protein intake, the response is similar regardless of age or sex.15,18
Children and adolescents. Strength gains in prepubertal children are real and substantial. The foundational meta-analysis of randomized trials in healthy youth found roughly 13 to 30% strength gains over 8 to 20 weeks of training.13 Adaptation is dominated by skill and neural drive with a smaller hypertrophy fraction that increases with maturation. Supervised resistance training is safe and beneficial; the American Academy of Pediatrics 2020 clinical report found no increased incidence of growth-plate injury in children weightlifting under proper supervision, and prospective injury rates from supervised programs run lower than common youth sports.14 The historical claim that lifting stunts growth is not supported by any prospective controlled study. For specifics on programming youth lifters, see our guide to youth resistance training.
Young and middle-aged adults. Peak strength typically occurs in the mid-20s, but the training response itself (how much strength a given dose produces from where you currently are) does not change much across the 20-50 range. Longitudinal data from powerlifters across multiple federations shows strength accruing through age groups with no abrupt inflection; performance trajectories are smooth functions of training age plus a shallow age-related modifier.15 A 45-year-old and a 25-year-old with the same training history, recovery, and nutrition will see comparable relative gains, even if the 25-year-old has a slightly higher absolute ceiling.
Older adults. The prescription that works for adults over 65 is essentially the prescription that works for adults under 65: progressive loading, multiple compound lifts, and adequate weekly volume distributed across two to four sessions (per the individual’s preference). Healthy older adults respond best to heavier loads. Most dose-response work centers around 70-80% of 1RM, but the LIFTMOR trial showed postmenopausal women tolerating sets of five at 80-85% of 1RM with strong adaptation and one minor adverse event across more than 2,600 sessions.7 Higher-intensity training consistently outperforms moderate-intensity work in older populations.16
The Fiatarone trial referenced in the intro is the strongest test of this principle: nursing-home residents with a mean age of 90 gained 174% in quadriceps strength on eight weeks of high-intensity training.1 The adaptive processes persist across the lifespan.
Power (high velocity strength) matters because it declines faster than strength after midlife and is more strongly associated with falls, disability, and mortality than maximal strength alone. The practical answer is not a separate power-training day or plyometrics protocol. Lifting the concentric phase of each rep as fast as possible while staying in control outperforms slow-tempo training on the functional endpoints that matter: rising from a chair, climbing stairs, walking quickly.17 Good practice at any age.
For more on muscle and strength loss in aging and how training counteracts it, see our sarcopenia guide.
Women. Women respond to the same prescription as men. In direct comparisons, hypertrophy and lower-body strength gains run at the same rate in both sexes, and women gain upper-body strength faster than men in percentage terms.18 Powerlifting data across the lifespan shows women improving faster than men, with smaller declines in older age groups.15 Through and after the menopausal transition, muscle and bone loss accelerate, mostly because estrogen drops. Resistance training counteracts that loss, and the LIFTMOR data showed heavy lifting is safe and effective in postmenopausal women with low bone density.6
When progress stalls
Stalled progress for four to six consecutive weeks is a sign to look at the training load before looking at age, genetics, or hormones. Training load means the total amount of training being done plus its nature: the lifts being performed, the intensity, the volume, the proximity to failure, the frequency, and the rate of progression. All of those go into one bucket.
The most common reason a program stops working is that the training load is no longer appropriate for the lifter. There are a lot of ways that happens:
- The lifter overshot the prescribed RPEs and is now training too close to failure too often.
- Weekly volume is too low to drive further adaptation.
- Weekly volume is too high relative to what the lifter can recover from.
- The exercise selection no longer matches the goal.
- Progression has been forced past the lifter’s actual capacity.
Environmental inputs sit on top of all of that and can wreck even a well-built program: short or fragmented sleep, low protein intake, large caloric deficits, life stress, illness, or the cumulative effect of any of these together.
A stall is information about the prescription. Our free Training Plateau Action Plan walks through the same approach we use with coaching clients.
Free training resource
Stuck on your lifts?
If your squat, bench press, deadlift, or other main lifts have stopped moving, the Training Plateau Action Plan walks you through the most common reasons progress stalls and what to adjust first.
Long-term strength development
Measurable strength gains show up within several weeks of consistent training in adults at any age. The trajectory is steepest in the first six to twelve months, then flattens. Longitudinal data from competitive powerlifters shows roughly 7.5 to 12.5% strength gain in year one and roughly 20% by year ten, with the curve front-loaded.15 For most recreational lifters that translates to large early progress, slower middle progress, and small but real long-term progress that compounds across decades.
The lifters who keep progressing year after year share two traits: they show up consistently and they continue to adjust their training load to their current fitness level. Sustained, well-programmed training performed over the years produces more than short bursts of fury.
The reasons to stick with it extend beyond performance. People who do any resistance training are roughly 21% less likely to die from any cause during follow-up than people who do none, with additional benefits beyond aerobic exercise alone.19 A separate review of 16 long-running cohort studies (median follow-up 25 years) found 10-17% lower risk of all-cause mortality, cardiovascular disease, total cancer, and diabetes from muscle-strengthening activity, with the largest benefit at roughly 30-60 minutes per week.20 Where you land relative to the broader population is mapped out in our strength standards guide.
Frequently Asked Questions
Is it too late to start lifting?
No. Resistance training has produced robust strength gains in every adult population studied, including frail nursing-home residents in their 90s.1 Detection of progress takes longer in heavily trained lifters; chronological age plays a smaller role.
Can kids lift weights?
Yes, with proper supervision and programming. The AAP and ACSM both reject the claim that resistance training stunts growth.14 Strength gains in prepubertal children are real, dominated by skill and neural adaptation, and add a small but measurable hypertrophy fraction.13 See our youth resistance training guide for programming.
Does the prescription change for women?
No. The same prescription that drives strength in men drives it in women: progressive loading, multiple compound lifts, and adequate weekly volume. Through and after the menopausal transition, heavy resistance training becomes more important, not less, because of accelerated bone and muscle loss. The LIFTMOR data showed heavy lifting is safe and effective in postmenopausal women with low bone density.6
How heavy is heavy enough?
Most strength work should be between 65% and 85% of your one-rep max, or RPE 6 to 8 for sets of 3 to 8 reps. Hypertrophy work can run lighter or higher in reps as long as sets are taken close enough to failure to recruit the high-threshold motor units. Bone adaptation responds to higher relative intensity, with LIFTMOR using sets of five at greater than 85% of 1RM.6
How often should I train?
Two to four sessions per week is the productive range for nearly everyone. Frequency is mostly a way to distribute weekly volume across the week; whether you do two sessions or four matters less than whether the weekly volume lands in a productive range.
What if I have a chronic condition or am post-injury?
Resistance training is well tolerated across most chronic conditions and is the cornerstone of rehab for most musculoskeletal injuries once acute symptoms have settled. Programming should account for current capacity and any specific contraindications. If that is your situation, our coaching team handles it routinely.
How long does it take to get measurably stronger?
Most adults see measurable progress in the first several weeks of consistent training. The first six to twelve months produce the largest gains. After that, progress is real but slower and harder to detect without a longer time window.
What is the difference between beginner, intermediate, and advanced programs?
The labels match a program’s measurement window to a lifter’s training history. A true beginner can confirm progress session to session, so beginner programs adjust load on that timescale. A lifter with a year or so under the bar needs weeks to confirm progress, so intermediate programs check on that timescale. A heavily trained lifter needs months, so advanced programs use longer measurement windows and more deliberate fatigue management. The mechanisms producing the gain are the same throughout. What changes is how long it takes to see the gain above day-to-day variation.
What is the best strength training program?
The best strength training program depends on your training history, goals, schedule, and current fitness level. Beginners usually do well with simpler programs that progress more frequently, while trained lifters often need more deliberate management of volume, intensity, exercise selection, and fatigue. A good program is one you can perform consistently, recover from, and adjust as your strength improves.
References
The post Strength Training Guide: How to Get Stronger appeared first on Barbell Medicine.