Scientifically reviewed by Austin Baraki, MD, FACP
In Chicago in 1944, in an army hospital ward at Gardiner General Hospital, Thomas DeLorme experimented with a rehabilitation approach his colleagues considered unorthodox. The patient was Sergeant Walter Easley, a paratrooper who had ruptured both his anterior cruciate ligament and his medial collateral ligament when he landed wrong on a jump. Easley had been at Gardiner for more than six months following the standard rehabilitation protocols of the era: rest, heat, and light exercises designed not to “overtire” the injured muscles. His doctors had told him he would wear a brace for life. DeLorme’s instruction was the opposite of what Easley had been told for the previous six months: lift the most weight you can handle for seven sets of ten repetitions, and the weight goes up only after you master the current load for all seven sets.
Within a month, Easley’s brace was off. DeLorme published the protocol the following year and is credited with originating progressive resistance training as it is now practiced. Eighty years later, the framework that bears his lineage has lost the principle his patients actually trained under. Most modern strength programming prescribes load increases on a schedule, calibrated to which stage of training the lifter is supposedly in, rather than to what the lifter has demonstrated they can handle.
Progressive Loading, Part 3
This article continues our Progressive Loading series by addressing one of the strongest arguments against reactive loading: the idea that beginners, intermediate lifters, and advanced lifters need fundamentally different progression rules because their biology works differently.
The short version: the biology does not switch modes. What changes across a training career is the size of the remaining adaptation, the amount of noise around the measurement, and the time window needed to see real progress.
Start with Progressive Loading, then read Beyond Progressive Overload for the practical loading strategies this article builds on.
The lifter who is adding thirty pounds to their squat each month is called a novice. The same lifter a decade later, who is having a good year if they add ten pounds, is called advanced. The novice-intermediate-advanced (NIA) framework that runs most strength training programming uses those categories to make three connected claims. First, novices and advanced lifters are biologically different in the rate at which the underlying adaptive processes function. Second, that rate difference dictates the progression model: novices add weight session to session, intermediates week to week, advanced lifters month to month or longer. Third, the rate difference dictates program design, with different programs prescribed at each tier.
The first claim lays the groundwork for the rest. If the adaptive processes change rate at some boundary, the other claims follow. The five lines of evidence below show that they do not. The framework is built on a biological premise that the underlying physiology does not support, and the prescriptions that follow from that premise fail in predictable ways.
This is Part 3 of the Progressive Loading series. Part 1 established that loading should react to demonstrated adaptation rather than try to force it. Part 2 covered RPE-based autoregulation and double progression as practical tools for implementing reactive loading. Both articles described the principle and the tools, but neither one engaged in detail with the strongest counterargument: that beginners and advanced lifters might be sufficiently different in their underlying biology to justify fundamentally different programming. That is the case Part 3 addresses directly.
This article walks five lines of evidence: neural adaptation, muscle hypertrophy, connective tissue, bone, and the fatigue physiology that links them. All of the adaptations run at the same rate at year one and year ten. The differences between an untrained lifter and an advanced lifter come down to remaining ceiling, measurement noise, and required stimulus. Everything underneath is the same: the biology, the fundamentals of programming, how to progress.
Progress should be earned. Improved fitness comes first; the weight on the bar follows.
A given program can work or fail at any level of training advancement. The variable that determines which is whether the training load is appropriate for the lifter in front of you. A label of novice, intermediate, or advanced does not answer that.
What is “training age” actually measuring?
Two terms will do most of the practical work in this article: untrained and trained. Untrained means less than roughly a year of consistent exercise with progressive loading. Trained means everyone else. Training age is mode-specific, as someone can be “trained” when it comes to resistance training, while being “untrained” with respect to aerobic exercise and vice versa. Regardless, training age is the continuous variable that predicts how long an observation window has to be before an improvement in fitness is detectable above the noise of day-to-day variability.
The main difference between untrained and trained lifters is not which adaptive processes are running or how fast they’re working. The processes and their speed are the same, but because the trained lifter is closer to reaching their maximum potential, the observed adaptations are smaller, and they take longer to detect above the noise of human performance variability.
What does the Novice Intermediate Advanced model prescribe?
The framework’s three claims compound into a specific set of instructions. Novices add weight to the bar every session, often in five-pound increments, because they are biologically capable of session-to-session adaptation. Intermediates add weight every week, because their adaptation runs on a weekly clock. Advanced lifters add weight every month or every block, because their adaptation requires longer to accumulate. Each tier’s prescription is justified by the rate the framework attributes to the underlying biology at that stage.
| The NIA claim | What the article argues instead |
|---|---|
| Novices, intermediates, and advanced lifters adapt at categorically different biological rates. | The same adaptive systems are running throughout a training career. The detectable signal gets smaller as the lifter gets stronger. |
| Progression should follow the lifter’s category: session-to-session, week-to-week, or block-to-block. | Progression should follow demonstrated performance, not a preset calendar. |
| Each training tier requires a different type of program. | Programming variables are the same for everyone: volume, intensity, frequency, exercise selection, proximity to failure, and progression. |
| A stall means the lifter has outgrown the current program category. | A stall is usually a loading, recovery, measurement, or expectation problem — not proof that the lifter changed biological categories. |
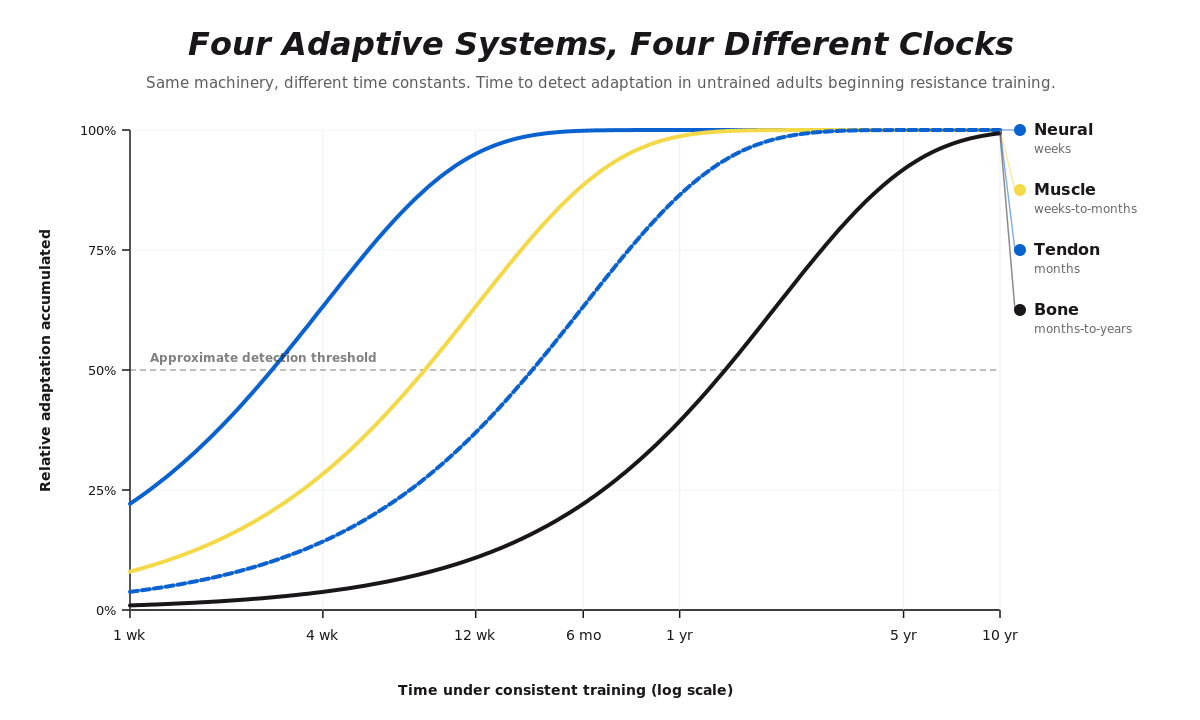
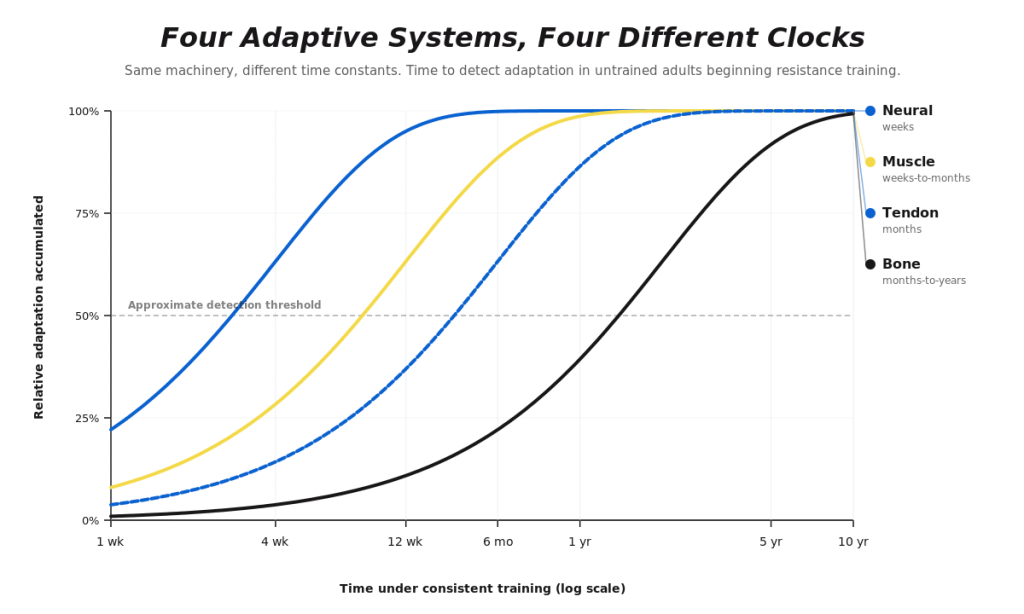
Figure 1. Four tissue-level adaptive systems on different time constants.
The key point from Figure 1
The issue is not that beginners and advanced lifters have different biology. The issue is that different tissues adapt on different timelines.
Neural adaptations can show up quickly, muscle growth accumulates over weeks to months, connective tissue often lags behind muscle, and bone remodels over months to years. A progression model that chases the fastest adaptation can exceed the tolerance of the slower systems.
Different progression schedules at each tier
The available data on time course of strength adaptation give a moderately predictable average with a wide range around it. A 2022 systematic review of 40 controlled training studies found that the average time to first detectable increase in 1RM or maximum voluntary contraction was 4.3 weeks, with individual studies ranging from one to twelve weeks.⁵⁶ Part of that range is an artifact of testing frequency: a study that does not test until week eight cannot detect changes that occurred earlier. The 4.3-week figure is when training studies on average first detected a significant increase, not necessarily when adaptation first occurred.
Trained and untrained populations in this review reached first-detectable strength gain on similar timelines, though the trained subgroup was small and the comparison was underpowered to rule out modest differences. The magnitude of gain at first detection differed substantially: untrained populations typically gain 15 to 30% on 1RM tests in 12 weeks, while well-trained lifters gain on the order of 2 to 6% per year on the same lifts.⁵⁷ The cleanest direct comparison comes from Ahtiainen and colleagues, who put eight strength athletes and eight non-athletes on identical 21-week programs.⁵⁸ Non-athletes gained 20.9% in strength. Strength athletes gained 3.9%.
Most of that gap reflects denominator math rather than a difference in trainability. A 5-pound gain on a 135-pound squat is 3.7%. The same 5-pound gain on a 405-pound squat is 1.2%. The absolute pounds added are identical and represent the same amount of new contractile capacity. The trained lifter is moving meaningfully more weight per session than the novice; the percent change is smaller because the baseline is much higher. Percent change against a moving denominator is a misleading way to track progress in trained lifters, and the article will return to this point in the classification section.
Day-to-day variability layered on adaptation uncertainty
The implication for NIA is not that strength adaptation is unpredictable. The problem is that there is a large variance in when the adaptation shows up, which is layered on top of another, large source of noise: day-to-day performance variation. Across sports, performance variability spans an enormous range.
The standard way to measure this is the coefficient of variation, or CV, which expresses how much an athlete’s performance bounces around from one competition to the next as a percentage of their average performance. A CV of 1% means an athlete’s performances cluster tightly around their average. A CV of 30% means they vary widely. Top international skeleton athletes have a competition-to-competition CV around 0.4%.⁶⁰ Top international surfers have a CV around 39%.⁶¹ Strength sports sit closer to the low end. Across 154 elite Olympic weightlifters competing internationally over the eighteen-month period leading up to the 2000 Sydney Olympics, the snatch CV was 2.7% for men and 3.7% for women, with comparable values in the clean and jerk and total.⁶² Test-retest CV in 1RM strength testing across populations runs in the same range, around 3 to 5%.³⁸ The same study found that lifters in the top half of each weight class had lower CVs than those in the bottom half.
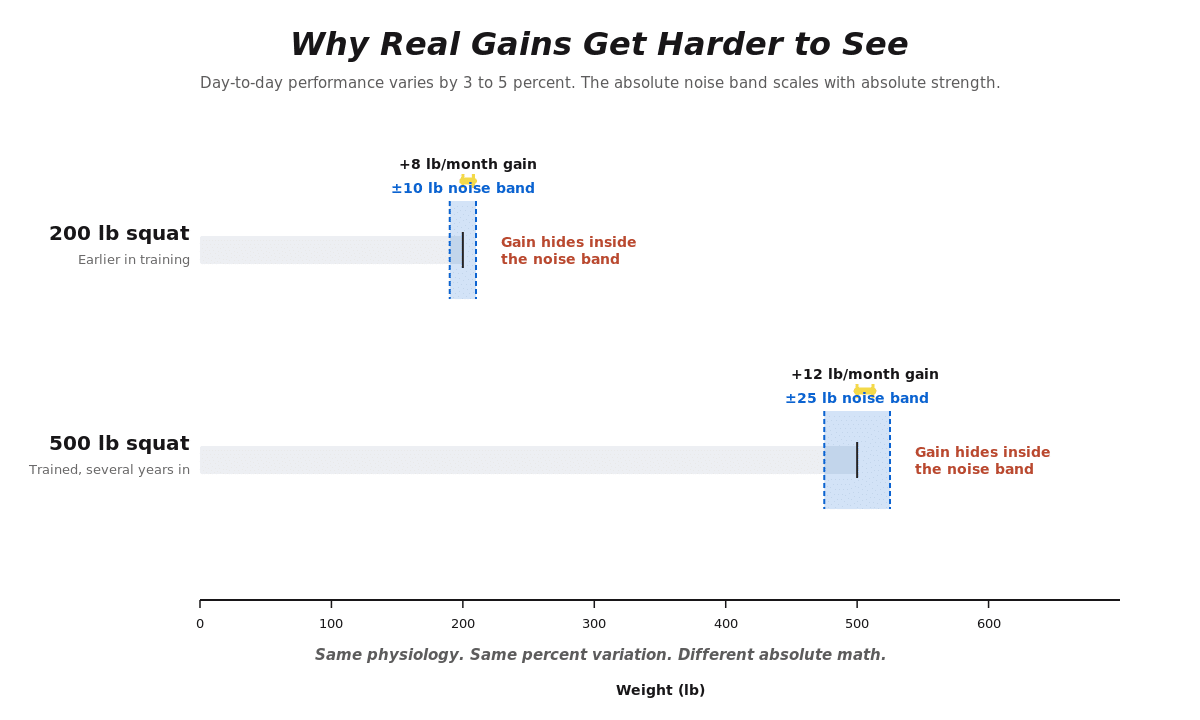
Figure 2. The same percent variation produces a wider absolute noise band at higher strength. Real gains can hide inside the noise.
Because the percent variation is broadly stable across populations, the absolute noise band scales with absolute strength. A lifter with a 500-pound squat has a day-to-day variation of roughly 25 pounds in each direction. A lifter with a 200-pound squat has a noise band closer to 10 pounds. A 2025 case series of seven physically active subjects who performed a true 1RM bench press every day for 38 days illustrates what that variability looks like in practice.⁵⁹ All seven improved their bench press by an average of nearly 30%. However, the findings beyond the average are more useful for an article about programming. One participant was weaker in week two than in week one, but the same subject went on to increase their bench by 23% overall. The participant who made the biggest absolute gain (70 pounds to peak) tested 20 pounds below their peak on the final day. The strongest subject in the study had the most day-to-day variability in their daily 1RM. The sample is small, but the observed variability is consistent with what really happens in the gym.
A prescription that adds weight every session is being applied on top of two sources of variance: the multi-week timeline of when the underlying adaptation shows up, and the day-to-day variation in overall performance. The schedule has no information about either. When the prescription lands correctly, the lifter is rewarded with a successful set, and the framework gets credit for predicting the adaptation. When it misses, the lifter either grinds through a set heavier than it should have been, generating fatigue without proportional adaptation; fails the lift and is told to deload, repeat, or reset because they have stalled; or underloads, because they have gained more strength than the prescription anticipated. All three responses treat the schedule as the truth and the lifter’s actual capacity as the deviation. The framework gets to be right whether or not its prediction was accurate, because the lifter is the variable that adjusts when the schedule and the biology disagree.
The Lambrianides review also found that studies adjusting training intensity throughout the program continued to show strength increases beyond the eight-to-twelve-week mark, while studies holding intensity at a fixed percentage of an old 1RM plateaued.⁵⁶ This is consistent with a real concern about loading too conservatively. A program prescribing 75% of an old 1RM works at first, but as the lifter gets stronger, the same absolute load becomes a smaller percentage of the new 1RM. The relative stimulus drifts downward and eventually falls below the threshold required to keep driving adaptation, which is roughly 70% of 1RM and above for strength.⁴⁵ A reactive approach is not a license to coast: if the load never moves, the lifter eventually trains below the intensity that produces adaptation in the first place.
Different programs at each tier
The framework’s claim isn’t only about how often to add weight. It also designates specific programming approaches to the different categories. Novices are prescribed “novice programs,” typically high-frequency, low-volume linear progressions. Intermediates are prescribed “intermediate programs,” usually weekly progressions with more volume and some structural variation. Advanced lifters are prescribed “advanced programs,” which the literature on this point gets vague about: the language tends to drift into terms like “more complex” or “higher volume” or “more variation,” without specifying what makes a program advanced beyond the implicit idea that it’s harder.
The underlying claim, when extracted from the language, is that the structural choices in a program (sets, reps, exercises, frequency, intensity distribution, rest periods) need to be categorically different at different tiers because the lifter’s biology requires it. The supporting evidence for this claim is thin. The dose-response literature on volume, frequency, and load shows continuous response curves rather than tier-specific patterns. Meta-analyses on training volume across training statuses find that more volume produces more growth and strength up to a ceiling, with the curve operating in similar fashion in trained and untrained populations.⁶³,⁶⁴ Frequency, when volume is equated, has minimal independent effect on adaptation in either trained or untrained lifters.⁶⁵
What does change with training status is the absolute volume the lifter tolerates, the absolute load they handle, and how close they are to their ceiling. There is no novice volume, intermediate volume, or advanced volume. The same is true for frequency, intensity, and total training load. These are individual variables, set by the lifter’s current tolerance, their goals, and the resources they have available. A label of novice, intermediate, or advanced tells you nothing about the individual’s exercise prescription needs.
What programming actually depends on
The fundamentals of programming are the same across the spectrum. Frequency, intensity, time, type, volume, and progression (FITT-VP) are the variables that get adjusted for any lifter at any stage. The general heuristic for hypertrophy and strength training is somewhere in the range of 10 to 20 working sets per muscle group or movement pattern per week, distributed across one or more sessions, with intensity above roughly 70% of 1RM for strength-focused work and a wider range for hypertrophy-focused work.⁴⁵,⁴⁶ Where any individual lifter sits within that range depends on their training tolerance, their goals, their available time, and what they have demonstrated about how they respond.
| Programming variable | What should determine it? |
|---|---|
| Volume | The lifter’s current tolerance, goals, schedule, and demonstrated response to prior training. |
| Intensity | The goal of the lift or session, the desired adaptation, and the lifter’s current performance capacity. |
| Frequency | Available training time, recovery resources, skill practice needs, and the total weekly workload the lifter can tolerate. |
| Exercise selection | The target adaptation, individual constraints, technical skill, preferences, equipment, and symptoms if present. |
| Proximity to failure | The desired training stress, the lifter’s recovery resources, and whether the session needs to build fitness or test it. |
| Progression | What the lifter demonstrates in training, not whether they are labeled novice, intermediate, or advanced. |
A novice running what NIA calls an “advanced” program will get good results if the training load fits them. An advanced lifter running what NIA calls a “novice” program will do well too, on the same condition. Either lifter on either program will fail when the training load is too low or non-specific to drive adaptation or too high to recover from.
The prescription critique above rests on a claim about what’s actually happening underneath. The next five sections walk that claim, starting with the nervous system.
Free download: Training Plateau Action Plan
If your lifts have stalled, the Training Plateau Action Plan helps you decide what to change first before jumping to a new program.
Use it to evaluate volume, intensity, frequency, exercise selection, technique, and recovery so your next adjustment is based on the problem you are actually trying to solve.
Neural adaptations
In a Harvard physiology lab in the late 1950s, Dr. Elwood Henneman watched electrical activity from the thread-like nerve projections of a cat’s spinal cord on an oscilloscope and noticed something peculiar. He was stimulating the sciatic nerve with electricity at increasing intensities and recording the readout from individual motor nerves. The small spikes always fired first. As he turned up the current, larger spikes joined in, never out of sequence, and never reshuffled. When he turned the stimulus back down, the largest units dropped out first and the smallest kept firing. First in, last out. Every time.
Henneman was not the first person to record the electrical activity from motor nerves, but he was the first to notice that the order was not random.⁴² Across different muscles and different stimulus types, the recruitment sequence held. By 1965 he and his colleagues had published a series of papers in the Journal of Neurophysiology establishing what he called the size principle: motoneurons are recruited in order of size, smallest to largest, because smaller cells need less input to fire, so they cross their activation threshold first. The implication was that the nervous system does not choose which motor units to fire. It chooses how hard to push, and the units fall in line according to a fixed hierarchy.
This is where most explanations of the size principle stop, and it is also where they go wrong. Recruitment order alone cannot account for the force a muscle produces. Once a motor unit, a single nerve and all the muscle fibers it connects to, is switched on, it can fire a few times per second or forty times per second, and that is the difference between a single twitch and a smooth, sustained contraction. Force output is the product of two variables: which motor units are active, and how fast each one is firing. Henneman gave us the first variable. The second is rate coding, and together they describe how the nervous system actually grades muscular force from a whisper to a maximal effort.
Strength is the force production capacity of the neuromuscular system in a specific context. How much force a lifter produces on a squat depends not only on how much muscle is available (the hardware), but on how effectively the nervous system can recruit and coordinate that muscle under load (the software). What training changes is the efficiency of the entire process: lower thresholds required to reach the high-threshold units, faster firing rates between contractions, better coordination between muscles pulling in the same direction, and more complete suppression of muscles that would otherwise oppose the movement. Training also raises the ceiling of motor unit recruitment under maximal effort and reduces antagonistic co-contraction, both of which contribute to strength gains without requiring more muscle.
These neural adaptations begin within the first sessions and continue throughout a training career. They are among the fastest adaptations in the system and among the first to go when training stops.2,3
How does muscular electrical activity change with training?
Voluntary movement starts as an electrical signal in the primary motor cortex. That signal travels down the spinal cord to a motor nerve, which branches out to connect with a group of muscle fibers. The nerve and the fibers it controls are collectively called a motor unit. Where the nerve meets the muscle, at a structure called the neuromuscular junction, the electrical signal triggers a chemical cascade that lets the contractile proteins inside the muscle fiber, actin and myosin, latch onto each other and pull. That pulling is what generates force. The whole sequence, from cortical signal to muscle contraction, is called excitation-contraction coupling, and the electrical activity along the way can be measured by placing electrodes on the skin over the muscle, a technique called electromyography, or EMG.
A study using high-density EMG technology in untrained subjects documented significant increases in motor unit firing rate and decreases in recruitment threshold within the first four weeks.⁴ These are the early-phase changes the standard textbook describes correctly. What the standard textbook gets wrong is the implication that the changes stop there.
When the quadriceps contract maximally, the hamstrings have to get out of the way. The spinal cord handles this automatically through a circuit that suppresses the opposing muscle the moment the prime mover fires. A 2025 review found that this suppression, called disynaptic reciprocal inhibition, is greater and faster in veteran strength-trained athletes than in recreationally active individuals.⁵ The practical consequence is that a larger fraction of the quadriceps’ actual contractile capacity reaches the measurement, because less of it is being canceled out by an antagonist that has not fully released. Adaptations of this kind take years to develop and cannot be attributed to muscle size alone.
Researchers compared three groups: people with four years of consistent resistance training, people with twelve weeks of training, and untrained controls. The four-year group produced agonist muscle electrical output at maximal voluntary effort that was 44% greater than the untrained subjects.⁶ That sounds like a cut-and-dried neural adaptation story, but as with most things in humans, it’s not that simple. Larger muscles generate larger electrical signals, so raw EMG differences between trained and untrained groups partly reflect the size of the muscle producing the signal, not the nervous system driving it. When voluntary EMG is normalized to the muscle’s own maximal electrical signal and properly controlled for muscle size, the difference between long-term trained and untrained individuals largely disappears.⁷ Neural adaptation continues beyond the early phase, but the magnitude is more modest than raw EMG comparisons imply.
How do new lifters get stronger so quickly?
Early gains in untrained lifters come from real adaptation, learning the movement, and getting better at the test itself, and the size principle only addresses the first.
A controlled trial randomized untrained men to either eight weeks of traditional resistance training or to repeating the 1RM test up to five attempts per session.⁸ The training group accumulated more volume and produced greater muscle growth at most measurement sites when compared to the 1RM group. However, changes in 1RM and force production were not significantly different between groups. To explain this finding, the authors concluded that there’s a familiarization period, where “practicing the test” improves someone’s performance. Another group of researchers argued that repeatedly performing a maximal effort constitutes low-volume, high-intensity training rather than mere test practice, and that the matched strength gains reflect a matched stimulus.⁹ Both positions have merit and both agree that the 1RM is partly a skill.
Henneman saw a fixed hierarchy in his cats. What he could not see from a single oscilloscope trace was that the same hierarchy gets fine-tuned over years of training. The available evidence suggests that the same neural processes are running at year one and year ten. The fast-acting components that show up loudly in the first month, recruitment threshold reductions and firing rate increases, are still running at year ten in the form of more efficient antagonist suppression and more complete voluntary activation. What looks like a fast adaptation that plateaus is actually a fast adaptation that shifts. Early gains include learning the test; long-term gains include circuits the textbook does not measure. The recruitment and rate coding mechanisms did not change modes. The detectable signal got smaller, and the components inside it shifted proportionally in what they contributed.
Muscle hypertrophy
In 1897, an Italian anatomist named Benedetto Morpurgo ran a small group of dogs on a treadmill for two months, then dissected their sartorius muscles and compared them under a microscope to the sartorius of untrained controls. The trained muscles were 13% larger by whole-muscle cross-section. The individual fibers inside them were 26% larger. The dogs had not grown new muscle fibers. They had grown the ones they already had. Morpurgo published the finding in a German physiology journal under a title that translates roughly to “On activity-induced hypertrophy of voluntary muscles,” and the central observation, that muscle growth is fiber enlargement rather than fiber addition, has held up across more than a century of follow-up work.⁴⁴
What Morpurgo could not see, and what he partly got wrong, was the mechanism. He attributed most of the fiber enlargement to expansion of the sarcoplasm, the fluid and non-contractile contents of the cell, rather than to the addition of new contractile protein. The next hundred years of work would establish that in response to mechanical loading, the dominant adaptation is the addition of myofibrillar protein, the actin and myosin that actually generate force. Morpurgo had the right phenomenon and the wrong driver. The driver was force.
Muscle growth happens when individual muscle fibers increase in cross-sectional area by adding contractile protein. The primary driver is mechanical tension, the force a muscle is required to produce during loading.¹⁰ When a muscle produces high force repeatedly, the mechanical signal drives the mTORC1 pathway and downstream protein synthesis, and the fiber grows over weeks to months.
Metabolic stress and muscle damage, once framed as independent drivers of hypertrophy alongside mechanical tension, are now understood as downstream correlates of the conditions that produce growth rather than independent causes.¹¹ Post-exercise spikes in testosterone, growth hormone, and IGF-1 do not predict hypertrophy or strength gains at any clinically relevant timescale.¹² Blood flow restriction training appears to work partly by forcing premature recruitment of high-threshold motor units under low mechanical load, which supports this interpretation: even BFR hypertrophy requires mechanical tension delivered through motor unit recruitment, not metabolite accumulation alone.
Why does muscle growth take so long to show up?
If mechanical tension is the signal, the next question is when it starts and how long it runs. The signaling cascade that drives protein synthesis activates within hours of a first training session, and the same cascade is firing throughout a training career.
What determines when growth becomes measurable is not when the process starts but when enough has accumulated to clear the noise floor of the measurement tool. The remaining ceiling shrinks across a training career, and the noise band on the measurement gets wider.
Two studies tracked this directly. A deuterium oxide labeling study, which tracks how much new protein the body builds over time, tracked ten weeks of training in untrained men alongside markers of tissue damage.¹³ At early timepoints, the rate of protein synthesis correlated with damage markers rather than with eventual muscle growth. Only after the body had stopped treating each session as a novel mechanical challenge did cumulative protein synthesis across the training block correlate with actual muscle growth almost perfectly (r = 0.94). A companion paper measured this directly in imaging data: thigh cross-sectional area rose 3 to 4% at week three, but much of that rise was fluid accumulation from tissue damage rather than new contractile protein.¹⁴ True growth reached 7 to 10% by week ten once the damage signal resolved.¹⁵
In trained lifters the detection timeline is longer because absolute gains are smaller, and between-subject variability is large enough that twelve-week changes below 3 to 5% may not clear measurement noise. A trained lifter who completes a twelve-week block and measures the same on imaging has not necessarily failed to grow. They may have grown and not moved the needle past what the instrument can distinguish from background variation.
Does the same muscle growth process really run forever?
The strongest version of the counterargument to the “same-process” framing is that the composition of what is available in the remaining ceiling may shift with training age. Type II muscle fibers, the larger, more powerful fibers recruited at high force demands, show roughly twice the hypertrophic response to resistance training compared to Type I fibers in most studies.¹¹ In untrained individuals these fibers sit well below their structural ceiling and respond robustly to loading. Whether a highly trained lifter who has been loading those fibers for years retains the same relative access to Type II fiber growth is uncertain.
Satellite cells, the muscle’s resident stem cells that contribute nuclei to growing fibers, predict hypertrophy magnitude in untrained individuals.¹² Those who show large satellite cell expansion and myonuclear addition tend to be extreme responders, and those who show neither tend to be non-responders. Whether highly trained lifters who have already been through multiple cycles of satellite cell activation and myonuclear addition retain the same responsiveness is not established in the human literature.
These are legitimate uncertainties, and they point to a continuous shift in what is available, not a categorical transition at any specific boundary.
Morpurgo could see the fibers got bigger, but he could not see the signal that told them to grow. A continuous shift in what is available with training age does not produce a kink in the adaptation curve, and it does not produce a moment when the lifter requires different programming because the underlying physiology has gone through a phase change. It produces a slow rebalancing of which contributions are doing how much of the work. The signaling cascade is the same in the trained lifter who has not seen a measurable change in cross-sectional area for half a year as it is in the new lifter at week one. The remaining ceiling is smaller, and the noise band is wider.
Tendons and ligaments
In 1999, in a sports medicine lab at Bispebjerg Hospital in Copenhagen, Henning Langberg and Michael Kjær did something nobody had done before. They threaded thin catheters into the tissue surrounding the Achilles tendon of a small group of marathon runners, just under the skin, and used them to sample the fluid bathing the tendon. The runners had just finished a 36-kilometer run. The catheters were a way of asking, in real time, whether the tendon was building new collagen in response to the loading. Collagen is the protein that makes up most of a tendon’s structure, and a rise in its building blocks in the surrounding fluid means the tendon is in repair mode. The signal did rise, but not on the timeline most readers would predict. It was still climbing 72 hours after the run. The tendon was responding, but it was responding slowly.⁵⁴
A follow-up study from the same group two years later tracked the same markers across eleven weeks of training and showed that the loading-induced increase in collagen turnover was still building at the eleven-week mark.⁵⁵ Muscle protein synthesis activates within hours of training, and the muscle tissue itself is measurably changing within weeks.
The connective tissue underneath runs on a slower clock. That lag is the mechanism behind almost every overuse injury in the first year of training, and it is why the lifter who is ready for more weight on the bar is often not yet ready for more force through the tendon.
How do tendons adapt to training?
Tendons attach muscle to bone and transmit contractile force into movement at the joint. Ligaments stabilize joints. Both adapt to mechanical loading by remodeling toward the demands they consistently experience, a principle articulated as Davis’s Law in the nineteenth century and now built out by the Berlin and Copenhagen tendon labs.
Two findings from this body of work matter for training. First, mechanical properties change before structure. A tendon gets stiffer and stronger before it gets thicker, because the changes happen at the molecular level inside the existing tissue before the tissue itself enlarges. Second, the loading has to be heavy. A pooled meta-analysis of 61 studies and 763 participants found that high-strain protocols, contractions at roughly 85 to 90% of maximum effort held for about three seconds, produced significantly larger gains in tendon stiffness than light-load training.¹⁶ The recommended dose for measurable adaptation is at least twelve weeks at this intensity.
Why does tendon adaptation lag muscle adaptation?
Achilles tendon stiffness determines how efficiently the force a muscle generates gets transmitted to the bone it moves. Stiffer tendons transmit force more efficiently without reducing flexibility or range of motion. In untrained adults, this stiffness takes roughly six to eight weeks of heavy loading to measurably change.¹⁷ In a longitudinal isometric calf training study, muscle strength rose significantly by two months while Achilles tendon stiffness did not reach significance until three months, with a 50% increase from baseline.¹⁸ Even under conditions designed to drive tendon adaptation, there is a six to eight week lag behind the muscle and neural changes.
The same pattern from strength and hypertrophy holds for tendons too: the closer the tissue is to its ceiling, the smaller the short-term response to a new intervention. The Lazarczuk meta-analysis noted that the three included studies recruiting well-trained athletes showed no change in tendon stiffness even with high-intensity training.¹⁶ The same machinery is running, but the room left for it to operate is smaller.
The lag between muscle capacity and connective tissue adaptation has direct consequences for how loading should progress in early training. The muscle is ready for more weight before the tendon is, and the gap between the two is what most early training-related injuries are made of. The traditional novice progression, which adds weight every session for as long as the lifter can recover between them, is calibrated to the muscle and the nervous system. The tendon is the system that does not get a vote in that calibration, and it is the system that fails first.
The same load:adaptation mismatch becomes most vivid at the extreme end. Anabolic steroids accelerate muscle protein synthesis substantially faster than tendons and ligaments can remodel. In one analysis of 22 tendon ruptures in weightlifters, 19 of the 22 occurred in anabolic users.²⁶ The engine became too powerful for the chassis. The same mismatch operates at smaller amplitude in any natural trainee whose load is climbing faster than connective tissue can adapt to it. Any scheduled load increase, whether session to session, week to week, or block to block, can produce the same mismatch. Loading has to be reactive to the adaptations the lifter has already acquired, at any cadence.
Langberg’s catheters caught the tendon mid-response three days after a single run, and the response was still climbing. The full adaptation to a training program takes months. The full adaptation to a training career takes years. The clock has not changed at year ten of training. The experienced lifter’s tissue is just further down the curve.
Why do beginners get hurt more than experienced lifters?
Resistance training has one of the lowest injury rates of any physical activity. Powerlifting sits at 1.0 to 4.4 injuries per 1,000 training hours across experience levels.²²,²³ Recreational running runs at approximately 10 or more per 1,000 hours. Within resistance training, there appears to be a difference between untrained and trained lifters that the NIA framework does not account for, and that connects directly to the connective tissue lag described earlier.
The most direct within-sport comparison comes from CrossFit. Novice participants in an eight-week program showed an injury rate of 9.5 per 1,000 training hours.²⁴ Experienced CrossFit participants doing the same type of training show 0.74 to 3.3 per 1,000 hours. A factor of three to ten within the same sport, the same movements, and the same general programming approach. The new trainees were not adequately prepared for the training being performed.
In powerlifting specifically, novice lifters are more likely to experience acute injuries, while experienced lifters are more likely to present with overuse injuries.²²,²³ Novices have accidents because they’re inexperienced. Experienced lifters develop overuse injuries when load:recovery mismatches accumulate. The underlying physiology is the same.
Most gym injuries are not structural catastrophes. They are overuse presentations: tendinopathy, muscle strains, nagging aches that developed over two or three weeks because volume or intensity climbed faster than the tissue could adapt. Available data show the average symptom duration for resistance training injuries is less than two weeks.²⁵ Disc herniations, torn ligaments, and structural failures keep people out for months. Injuries that resolve in days to two weeks are predominantly overextension of the adaptive budget.
A loading schedule that prescribes session-to-session weight additions because the trainee is “still in the novice phase” often overextends that budget. The schedule is an artifact of the starting condition. A novice who begins well below their actual capacity can add weight session to session for a while because they’re climbing back to where they already were. Some of that climb is real strength adaptation. Some is the lifter expressing capacity they already had. Either way, the schedule looks like progress, and the framework gets credit for predicting it. When the runway runs out, the schedule keeps prescribing weight additions on the same cadence, and the lifter has to grind, stall, or get hurt to demonstrate that the cadence was never tied to anything underneath.
Load tolerance is itself an adaptation. The experienced powerlifter handles absolute loads that would hurt an untrained person because they have built that tolerance over years, in the same muscle, tendon, ligament, and bone the novice has. There is no separate “experienced lifter physiology” doing the work. The pace at which load can climb is set by the tissue that adapts slowest, which in early training is connective tissue.
Bone
In 1892, the German anatomist and surgeon Julius Wolff published a monograph in Berlin called Das Gesetz der Transformation der Knochen, “The Law of Bone Transformation.” Wolff had spent years cutting open human femurs and looking at the internal architecture of the bone in cross-section. The femoral neck, the angled section that connects the long shaft of the femur to the ball of the hip joint, was not solid. It was a lattice of bony struts, called trabeculae, oriented in specific directions. Wolff compared the pattern of those struts to a drawing the engineer Karl Culmann had published in 1866 of the stress lines inside a curved mechanical crane designed to carry load through a similar bend. The two patterns were nearly identical. Wolff’s conclusion was that bone, like the crane, had its internal architecture organized along the lines of the forces it was required to carry, and that this architecture would reorganize over time if the forces changed.²¹
Wolff got the broad principle right and some of the details wrong. The modern picture is that bone deposits material where load demands it and resorbs material where load is absent, and that this remodeling happens through a coordinated cycle of cells that build bone (osteoblasts) and cells that break it down (osteoclasts). What Wolff could not have known is how slowly the cycle runs. A complete bone remodeling cycle takes three to six months. DXA-detectable changes in bone mineral density typically require six to twelve months or more of well-prescribed loading to register.¹⁹
How does bone adapt to training?
The LIFTMOR trial enrolled postmenopausal women with low bone mass and assigned them to either eight months of twice-weekly heavy resistance and impact training or to a low-intensity home exercise control. The training group gained roughly 4.1% in lumbar spine bone mineral density and 2.2% in femoral neck bone mineral density compared to controls.²⁰ Eight months of consistent, heavy loading. A few percentage points on a scan. That is what a successful bone adaptation looks like on a measurement tool, and it is the most positive trial result in the resistance training and bone literature.
Bone responds to two features of mechanical loading: how heavy the load is, and how quickly the load is applied. Heavy and dynamic beats light and slow. This is why high-velocity impact and heavy resistance training together produce larger effects than either alone, and why walking, while valuable for many things, does not appreciably build bone in adults who can already walk. The osteogenic stimulus is calibrated to forces that exceed the bone’s habitual loading, and the bone of an adult who walks every day is already adapted to walking.
For a deeper look at osteoporosis and how resistance training fits into prevention and treatment, see our guide to osteoporosis.
Why doesn’t bone adaptation show up in normal training timelines?
The cycle is slow, the detectable signal is small, and the measurement tool has a noise floor. A DXA scan is precise enough to detect meaningful changes over six to twelve months, not over a training block. A lifter who runs a twelve-week program and gets a DXA at the start and end will see a number that is dominated by the scanner’s measurement variation, not by anything the training did or did not do. The signal exists. It is below the floor of what the instrument can resolve in that window.
This is the same pattern that runs through the rest of the article, scaled up in time. The cell biology has not changed. The remaining ceiling and the noise band are working at a longer timescale than they do for muscle or tendon. Bone is the slowest of the four clocks, and no realistic training block resolves it inside a window a coach can use to make Tuesday’s load decision.
Wolff saw the lattice of struts inside the femoral neck and recognized that bone was an engineered structure. He could not see how long the engineering took. The same osteogenic cascade is running in the lifter at week one and the lifter at year ten. The detectable signal is small enough that no realistic training block produces a DXA change a clinician can interpret session by session. The process is doing its work, but it does not produce a number a coach can use to make Tuesday’s load decision.
Fatigue
In 1884, in a physiology laboratory at the University of Turin, Angelo Mosso clamped a subject’s forearm into a wooden frame, isolated the middle finger, attached a small weight to it by a cord over a pulley, and asked the subject to lift the weight repeatedly until the finger could no longer move it. A stylus traced each contraction onto a rotating drum of smoked paper, producing a curve that flattened over time as the finger fatigued. Mosso called the instrument an ergograph and the curves it produced ergograms, and he spent the next twenty years using it to study how human beings get tired.
Two findings from this work matter for the modern picture. First, every subject had a different fatigue curve, and the curve for any one subject changed depending on the conditions of the test. Fatigue was not a single number that described how tired someone was. It was a pattern that depended on what the subject was doing, what they had done recently, and what was happening in the rest of their body and mind. Second, Mosso tested two professors with his ergograph immediately after they had each given a long lecture. Their finger endurance was measurably reduced compared to baseline. The professors had not used their fingers during the lecture. Something about the work of speaking and thinking had reached the muscles of the hand. Mosso’s interpretation, in 1891, was that fatigue was at least two distinct things: a peripheral process in the muscle and a central process in the brain. He was right, and the modern fatigue literature has spent the better part of a century building out the taxonomy he opened.⁴³
If neural drive, hypertrophy, connective tissue, and bone all run identically at year one and year ten, the way training feels at different career stages should reduce to the same physiology applied at different absolute loads with different calibration. It does. Fatigue is the fifth evidence stream for the same-machinery argument, and it is the one where the NIA framework borrows the most apparent traction, because the framework attributes the way training feels at different career stages to a categorical biological difference. Most of what is actually different is the lifter’s calibration to the same set of underlying processes.
What is fatigue?
Most of what gets called “fatigue” in the gym is at least four different things. Treating them as one thing is where a lot of bad programming logic gets imported under the cover of biological-sounding language. The contemporary taxonomy, anchored by Enoka and Duchateau, separates fatigue into dissociable phenomena.²⁷,²⁸
- Performance fatigability is the objectively measurable acute decline in force, power, or velocity output during or after a task.
- Perceived fatigability is the moment-to-moment subjective sensation of effort, discomfort, and tiredness that accompanies the task.
- Trait or state fatigue is the longer-duration self-reported symptom of tiredness or exhaustion that exists independent of any specific task.
- Recovery state and accumulated training stress is an integrated construct describing where someone sits on the acute-fatigue, functional overreaching, nonfunctional overreaching, overtraining syndrome continuum.²⁹
These four constructs are correlated, but not interchangeable. A lifter who slept poorly and is anxious about a session has elevated perceived fatigability. If the session is a one-rep max attempt, perceived fatigability may have little leverage on performance because the task ends before perceived effort accumulates to a behaviorally limiting level. The lifter feels poor but still manages to lift well. Conversely, a lifter who is in the middle of a high-intensity training block may have reductions in muscle contractile function or impaired recruitment that show up as an excessive velocity drop within a set or reduced weight at a given RPE. The lifter feels fresh but lifts poorly. This model of fatigue explains both patterns. NIA, which inherits from a stress-recovery-adaptation framework that treats fatigue as one thing to be “recovered from,” does not.
What does the 1RM actually measure?
The fatigue section showed that what the lifter feels is the sum of several distinct processes. The number on the bar is also the sum of several different processes. Strength, when represented by a single number like a 1-Repetition Maximum (1RM) test, is the integrated output of all four adaptive systems, plus the lifter’s skill on the test, the lifter’s calibration to maximum effort, and the environment. Training changes all of those simultaneously, except the environment. The 1RM is the integrated readout.
The 1RM is a reliable test. Tested twice in similar conditions, a lifter’s number stays consistent. Intraclass correlation coefficients run from 0.90 to 0.99, and day-to-day variation clusters around 3 to 5% in most populations. A systematic review of 32 reliability studies found that in 34% of analyses, retest values were systematically higher than initial values, with the gap averaging roughly 4 to 12 pounds upper-body and 10 to 12 pounds lower-body.³⁸ That gap represents the test improving with repetition independent of whether the trainee has gotten physiologically stronger.
The squat and deadlift are technically demanding movements. Early performance improvements on them reflect a mixture of better movement coordination, increasing familiarity with producing true maximal effort, and actual changes in neuromuscular capacity. A protocol in which trained lifters worked up to a heavy single or near-maximal set within a prescribed effort range across consecutive training days produced strength gains that rivaled or matched higher-volume approaches.³⁹ Skill accumulation on the specific movement was part of the mechanism alongside genuine physiological adaptation.
In a 12-week trial of 33 men’s elbow flexors with a preceding familiarization period, hypertrophy explained roughly 25% of individual variance in isometric strength gain and even less in 1RM gain.⁴⁰ A separate cross-sectional comparison found that trained men with roughly 50% greater knee extensor strength than untrained controls had that advantage almost entirely explained by larger quadriceps volume, with modest contributions from muscle architecture and specific tension.⁴¹ Gaining muscle and gaining strength are related but distinct outcomes. A 1RM is a composite readout of neural, architectural, morphological, and skill factors simultaneously, and short-window 1RM observations capture all of that noise at once.
Early strength gains are a composite signal.
RPE and RIR are calibration skills
The NIA framework typically claims that experienced lifters tolerate more, recover faster, or experience fatigue qualitatively differently than novices. The biology hasn’t changed. What experienced lifters have is a better-tuned sense of what loads should feel like.
Using Rating of Perceived Exertion (RPE) and repetitions in reserve (RIR) to determine exertion is anchored to an individual’s prior experience with failure.³⁰ A scoping review of accuracy in predicting repetitions to failure found that lifters across training experience levels under-predict reps to failure by approximately 2 to 5 reps on average, with only a tendency toward improved accuracy in more experienced trainees.³¹ The variable that drives accuracy is not necessarily training age. It is recency of practice with the scale itself. A lifter who recently took a set to failure reports RPE 9 close to true 1 RIR. The same lifter, six months later without performing a set near failure, is likely to be less accurate regardless of training age.
RPE accuracy is a skill that develops with use. Novices who receive instruction in RPE and practice it during training improve their accuracy on the order of weeks, not years. A direct head-to-head study of trained versus untrained lifters on the back squat in a Smith machine format found no statistically significant difference in RIR accuracy between groups.³²
The NIA-derived position that novices can’t use RPE because they won’t pick the “right” weight is unserious. Almost all novices on NIA-style programming start with an artificially light weight and then proactively add weight too quickly, which is the same imprecision that RPE is being accused of. The biggest health benefits from lifting occur when going from no lifting to some, which makes the difference between picking the “right” weight and a “good enough” weight inconsequential for long-term outcomes. The viable intensity range for adaptation is wide enough that being a bit off doesn’t materially change the result. At worst, RPE underloads an untrained person for a brief period when the main goal is getting them lifting at all. A rigid schedule for adding weight can put someone on the couch instead of in the gym.
Recovery converges in two to six weeks
The repeated bout effect is the clearest training-status difference in acute recovery. Untrained subjects performing eccentric-biased or novel exercise show pronounced soreness, larger creatine kinase rises, larger force decrements, and slower force restoration after a first bout.³³ After a few exposures to the same stimulus, the response attenuates substantially. The functional consequence: an untrained lifter doing their first set of squats has larger, longer-tailed recovery demands than a veteran doing the same relative effort. After roughly two to six weeks of consistent training, the untrained lifter’s recovery kinetics begin to resemble those of trained populations for that specific stimulus.³³
The implication is that “novice recovery” in any meaningful sense lasts about a month and a half. After that, the same recovery physiology that runs in the trained lifter is running in the new lifter, attenuated only by the absolute loads in play and the lifter’s calibration of what hard means. Training programs that prescribe vastly different recovery architectures for novices versus advanced lifters are responding to a six-week phase as if it were a permanent biological condition.
Heavy training does not “fry” the central nervous system
The claim that advanced lifters are limited by accumulated CNS fatigue, and therefore require categorically different programming, has been tested directly. Skarabot and colleagues assessed neuromuscular fatigue and recovery after heavy resistance training (10 sets of 5 back squats at 80% 1RM), jumps, and sprints in trained men using femoral nerve electrical stimulation and transcranial magnetic stimulation.³⁴ All three modalities produced fatigue requiring up to 72 hours to fully resolve. The etiology was predominantly peripheral, not central. Cortical output never showed the deficit the standard narrative predicts. The fatigue that resolved over 72 hours was in the muscle and its connective tissue, not in the brain.
Heavy low-rep work is not categorically more “stressful” than higher-rep work. Within a session, lower-load sets taken to failure produce greater discomfort, greater perceived fatigue, greater HRV depression, and greater acute force decrements than heavy low-rep work performed below failure.³⁵ A 3×3 at 90% with 1 to 2 RIR per set is, for many trained lifters, less acutely fatiguing than a 3×12 at 70% taken to failure.
The framing that heavy training uniquely affects the CNS is wrong. Training to failure is what produces disproportionate fatigue, and NIA’s prescriptive schedule pushes lifters there routinely.
Are minimum effective dose and maximum recoverable volume useful?
NIA-style programming claims that the minimum dose required to produce adaptation rises across training tiers. Novices grow on a few sets per week. Intermediates need more. Advanced lifters need substantially more to keep responding. This dose-response pattern is supported by data, where the more experienced lifter generally needs more training to see a result. That said, there are no distinct boundaries that identify the increased need and there are large differences between individuals with the same experience level.
The training load an individual needs is not predicted by a categorical label. The novice has a wide gap between zero training and their adaptive ceiling, so a small dose produces a large response. The trained lifter is closer to their ceiling, so the same dose produces a smaller response and they need more total work to extract the next increment of adaptation. The relationship between volume and hypertrophy is non-linear: at the high end of the volume range, more volume produces diminishing returns, and in some studies produces no hypertrophy at all compared to moderate volumes.³⁶ The curve is the same. The lifter’s position on it is what changes.
The upper bound of this same framework is sometimes invoked as maximum recoverable volume (MRV), the volume above which the lifter cannot recover. MRV is conceptually equivalent to overreaching and is not related to the volume that actually optimizes hypertrophy. A lifter could regularly perform and recover from very high volumes that exceed what would be optimal, or have a recuperative capacity poor enough that their MRV sits below their optimal volume. The two are dissociated.³⁶ The dose-response literature also doesn’t support progressing volume proactively across a mesocycle. Volume comparisons are based on total volumes across training durations, not week-to-week escalations, and no study has matched total volume while comparing a group that increases weekly sets to a group that holds sets constant.³⁶ Progressive overload should be reactive, with load or volume increasing when the lifter has demonstrated the capacity to absorb the change.
When NIA proponents are pressed on what advanced lifters actually need more of beyond volume, the specifics get vague fast. More complexity, more programming sophistication, more variation. There is no published evidence that “complexity” is a meaningful programming variable, and no operationalized definition of what makes a program advanced.
The real programming question is simpler. Training load is the integrated product of volume, intensity, exercise selection, proximity to failure, and frequency. The coach’s job is to maximize the training load that fits the individual lifter. The two real bottlenecks are time, which is a logistical constraint, and physiology, which is the lifter’s tolerance and recovery capacity. Both vary continuously across lifters at every training age. Neither maps to a category.
Some lifters with three years of training tolerate more weekly load than other lifters with ten. Some advanced lifters have hour-a-day schedules and need programming that fits sixty minutes. The training load that maximizes adaptation under those constraints isn’t a function of which tier the lifter belongs to. It’s a function of who the lifter is and what they have to work with.
Tracking how a lifter is responding to that load uses the same five constructs at every training age: performance fatigability, perceived fatigability, recovery kinetics, central versus peripheral contributions, and the room to push past the lifter’s effort anchor. Subjective wellness questionnaires outperform most commonly used objective tools for tracking longitudinal training response.³⁷ Velocity loss and RIR provide the most direct in-set proxies of acute performance fatigability. A “feel bad, lift well” or “feel fresh, lift poorly” day should be treated as data and used to inform load selection. The tools that work for the experienced lifter are the tools that work for the novice. Same physiology, different position on the same curve.
What is the Novice-Intermediate-Advanced system categorizing?
Nothing in any of the five lines of evidence justifies a categorical biological transition between novice, intermediate, and advanced. The Latella retrospective of more than 9,000 powerlifters shows a smooth, logarithmic curve from year one through year ten with no visible inflection at any of the framework’s tier boundaries.¹
What the labels actually encode is a detection problem. Strength performance varies by approximately 3 to 5% from session to session in well-trained athletes, driven by fluctuations in sleep, motivation, nutritional status, the environment, and stress.³⁸ This is the noise floor of the measurement. It does not shrink with better programming or more consistency, and it does not respond to category labels.
That 3 to 5% scales up with absolute strength. A lifter squatting 500 pounds varies by roughly 25 pounds in each direction from session to session. Monthly gains of 2 to 3% at that strength level produce 10 to 15 pounds over four weeks, which is smaller than the day-to-day variation. The window required to confirm genuine adaptation gets longer as the lifter gets stronger.
People often interpret this as “my training stopped working.” The gains got smaller relative to the noise, the readout looked flat, and the lifter or the coach concluded the program had run its course. The standard response is to switch to a different program, usually one labeled for the next tier up. The switch solves nothing, because nothing was wrong with the previous program. The lifter was adapting; the adaptation was just smaller than the day-to-day variation, and the window for evaluating it was too short.
In medicine, treating a lab value and treating the disease it reflects are often different interventions. The number on the page is reporting on something deeper, and buffing the chart does not fix the underlying process. The weight added to the bar per session is not the adaptation. It is a readout of the adaptation, subject to noise, timing, and measurement constraints. Switching programs because that readout looked flat for three weeks is solving a measurement problem with a training intervention.
The NIA labels track how often a lifter’s gains are large enough to be obvious. The novice puts five pounds on the bar every week. The intermediate puts five pounds on the bar every month. The advanced lifter puts five pounds on the bar every few months. The categories track the same physiological process at three different distances from a ceiling. As the lifter approaches the ceiling, the same five pounds of new strength takes longer to accumulate above the noise.
The NIA labels are positions on a single trajectory without hard boundaries. A framework that believes in boundaries that aren’t there fails in predictable ways. It misidentifies the biology, claiming that “new” adaptive processes come online at each tier when the same processes are running throughout. It prescribes loading proactively, treating adaptation as something the schedule can predict in advance, which conflicts with the wide variability in how individuals adapt and how they perform on any given day. The result is loading that isn’t matched to the lifter, which can produce both over- and under-loading. It fails at program design because no categorical label answers the questions that actually determine what a lifter needs: how much training load does this individual need, and what should it be made of?
What does reactive programming actually look like?
The replacement for the NIA framework requires a different orientation toward programming decisions: reactive rather than proactive, driven by what the lifter demonstrates rather than by what a category implies should be happening. The reactive label and the practical application of RPE-based load selection in strength training owe a meaningful debt to Mike Tuchscherer of Reactive Training Systems, whose manual from the late 2000s brought these tools into mainstream powerlifting.
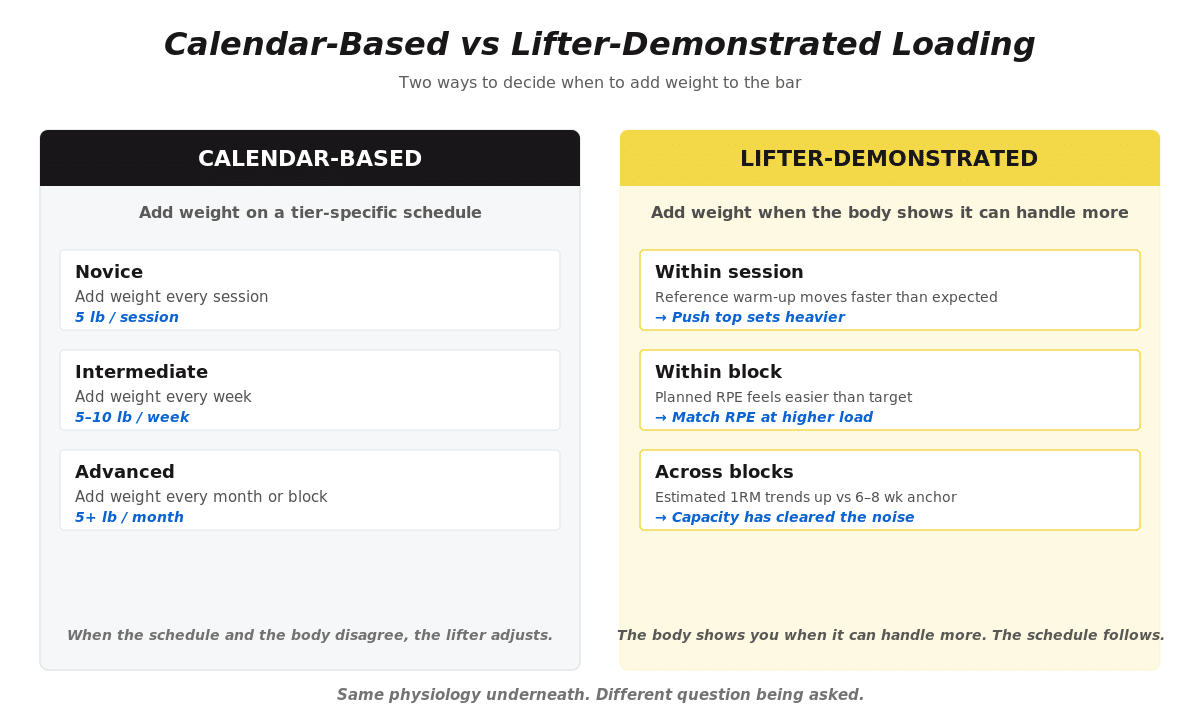
Figure 3. Calendar-based programming vs lifter-demonstrated programming.
A trust-the-process argument needs a falsification criterion. The answer is not time-based. It is load-based, and understanding why requires knowing how wide the viable training load range actually is.
For strength development, intensities of approximately 70% of 1RM and above produce similar outcomes across most well-powered comparisons.⁴⁵ For hypertrophy, the range is wider still: nearly any intensity produces meaningful muscle growth if proximity to failure is adequate, which is why blood flow restriction training at 20 to 30% of 1RM can drive hypertrophy when effort is sufficient.⁴⁶ This width matters because moderate deviations from optimal loading in either direction do not cost much. A lifter training at 72% instead of 78% with the same proximity to failure and total volume is operating at a different point inside the same viable range, with similar outcomes expected.
Reactive loading in practice
The question is not, “What category of lifter am I?” The better question is, “What has my recent training shown I can handle?”
- Warm-ups feel lighter and faster than expected: consider increasing load for the day’s top sets.
- Warm-ups feel about the same: repeating the prior load may be the correct decision.
- Warm-ups feel noticeably slower or heavier: preserve or reduce load to keep the intended training stress in range.
- Performance has been flat for several weeks: evaluate the trend, recovery inputs, and training load before changing programs.
A genuine stall worth doing something about can’t be diagnosed from a few flat sessions alone, as the adaptation may be lurking within the noise band. Once sleep, protein, and life stress are accounted for, a continued absence of progress raises the probability that the training load itself is the problem. Two failure modes drive most real stalls. The first is a training load that has drifted below the threshold required to keep driving adaptation. The second is a training load that has climbed faster than the lifter has actually adapted. Both produce a flat readout. The diagnostic question is which one, and the rest of this section walks the signals that distinguish them.
Within the session: what does the warm-up tell you?
The most reliable within-session signal is the warm-up. Even a lifter without a single repeated reference weight has done warm-ups close enough to today’s, week over week, to have a rough expectation of what each should feel like. A new lifter builds that expectation in their first weeks of training by working up to weights at different effort levels and developing a sense of what each feels like. Once the expectation exists, the warm-up either lands in the expected ballpark or it doesn’t.
If the warm-ups feel lighter and faster than expected, performance potential today is high and there is real evidence to push the top sets heavier. If they feel noticeably harder or slower than expected, performance potential is suppressed and adding weight is likely to generate more fatigue than adaptation. The honest comparison is what the warm-ups actually felt like, not what the lifter wanted them to feel like.
Add weight when the new strength has declared itself. Repeat or reduce when it has not.
Over time: what counts as a genuine stall?
A genuine stall worth investigating is a lack of demonstrable improvement in a priority lift over three to four weeks, with consistent training, adequate sleep, adequate protein, and manageable life stress in place.⁴⁷ That three to four week estimate scales in both directions. Lifters with less training history may show demonstrable changes sooner. Lifters with more training history may need a longer window. The comparison that matters is against a recent anchor, the best performance of the past six to eight weeks, not a lifetime best.
Estimated 1RM from sets performed within a consistent rep range at consistent RPE targets is more useful for ongoing monitoring than tested maxes, because it does not require a dedicated test session.⁴⁷ When rep ranges or RPE targets are variable, the signal becomes too noisy to interpret. In that case, a single at RPE 8 or a triangulation approach (performing the same exercise at RPE 7, 8, and 9 at the start and end of a block) provides a cleaner comparison.
| Signal | More likely interpretation | First move |
|---|---|---|
| Warm-ups feel normal, but top sets are not improving over several weeks. | The training dose may no longer be enough to drive adaptation. | Consider a small increase in training load, usually through volume, frequency, or exercise exposure. |
| Every session feels like a grind, soreness is persistent, and performance is flat or declining. | Training stress may be too high relative to recovery. | Reduce training load temporarily while preserving the main movement pattern. |
| Sleep, nutrition, or life stress has recently worsened. | The environment may be limiting performance expression. | Adjust expectations and avoid adding more training stress to compensate. |
| A few sessions are flat, but training quality is otherwise good. | This may be normal measurement noise. | Stay the course and compare against a recent multi-week anchor, not a single day. |
When training load is within the viable range and the environment is supportive but progress has genuinely stalled, the investigation follows a sequence. First, is the issue more likely insufficient stimulus or insufficient recovery? A trainee who feels fresh, motivated, and not particularly sore but whose numbers are flat is probably under-stimulated. A trainee who is sore more often than not, whose motivation is declining because every session grinds, and whose joint discomfort has increased is probably over-reached. Session RPE tracks this. Consistently below 6 or 7 suggests training load is too low. Consistently above 8 with flat or declining performance suggests it is too high.
Second, has the environment changed? Sleep, protein and Calorie intake, and life stress are the primary variables. When any of these is meaningfully compromised, the expectation of progress should change, and the appropriate response is reduced training load to maintenance levels rather than increased training load to compensate. Adding training stress on top of life stress produces more fatigue, not more adaptation.
Stalled right now?
The Training Plateau Action Plan gives you a step-by-step framework for deciding whether to adjust volume, intensity, frequency, exercise selection, technique, or recovery.
What about detraining?
The same logic that makes the adaptation curve smooth in one direction makes it smooth in the other. If the underlying processes do not switch modes when adding load, they do not switch modes when load is removed. Strength is more durable than most lifters expect.
In resistance-trained men, two weeks of complete cessation produces no measurable strength loss.⁴⁸ A meta-analysis of more than 100 detraining studies found strength loss minor or absent for approximately 28 days of complete cessation.⁴⁹ What decays first is the nervous system’s contribution. Maximal muscle electrical activity decreases before morphological changes appear, suggesting the neural layer is the most volatile component of strength, sitting on top of a more durable structural substrate.⁵⁰ Rate of force development appears to be maintained during detraining, so the pattern applies specifically to maximal strength expression rather than all neural adaptations uniformly.⁵¹
The most striking detraining data comes from a study of older adults who trained intensively for two years and then stopped for three years. Five years after they started, three years after they stopped, their leg press and bench press maxes were still 14% and 9% above where they began.⁵² Three years without training and still meaningfully above baseline.
Consistent training compounds. The adaptive base built over years does not evaporate when life gets complicated. It decays slowly, on the same asymptotic curve that built it. Older adults lose strength faster during cessation than younger adults and require a higher maintenance dose, typically two sessions per week.⁵³ Younger adults can maintain strength for many weeks on as little as one session per week and one set per exercise as long as relative intensity is preserved. Same processes, same direction of decay, different absolute rates depending on age and absolute strength level.
Key takeaways
-
The novice-intermediate-advanced framework treats a measurement problem like a biological category.
The adaptive systems do not switch modes across a training career. -
Progression should be reactive at every stage.
The load should increase when the lifter has demonstrated the capacity to handle more. -
Different tissues adapt on different timelines.
Neural adaptation can show up within weeks, muscle growth accumulates over weeks to months, connective tissue often takes longer, and bone remodels over months to years. -
Early-training injuries are often load-tolerance problems.
Muscle and neural improvements can outpace connective tissue adaptation when loading climbs too quickly. -
A real stall is diagnosed from trends, not a few flat sessions.
Compare recent estimated 1RM trends against a six-to-eight-week anchor while accounting for sleep, nutrition, life stress, and training load. -
Strength is more durable than most lifters think.
The adaptive base built over years decays gradually, not instantly.
What to do next
Do not choose a program or progression model because a label says you are a novice, intermediate, or advanced lifter. Choose the training load that fits your current capacity, goals, schedule, and demonstrated response.
-
Want a structured program?
The Barbell Medicine strength templates are designed around these principles. Pick the template that fits your schedule and current capacity, run it for the prescribed block, and let the loading react to what you demonstrate in training.
View Barbell Medicine strength templates -
Want individualized programming?
The Barbell Medicine coaching team works from your actual training history and adaptive response rather than a tier label.
Apply for coaching -
Working through a stall?
Download the Training Plateau Action Plan for a step-by-step framework to evaluate volume, intensity, frequency, exercise selection, technique, and recovery.
Download the Training Plateau Action Plan
Continue the Progressive Loading series
This article is Part 3 of the Progressive Loading series. Start with Part 1: Progressive Loading, then read Part 2: Beyond Progressive Overload for the practical loading strategies this article builds on.
References
- Latella C, Steele J, et al. Using powerlifting athletes to determine strength adaptations across ages. SportRxiv. 2023. https://doi.org/10.51224/SRXIV.250
- Sale DG. Neural adaptation to resistance training. Med Sci Sports Exerc. 1988;20(5 Suppl):S135-145. PMID:3057313
- Moritani T, deVries HA. Neural factors versus hypertrophy in the time course of muscle strength gain. Am J Phys Med. 1979;58(3):115-130. PMID:453338
- Del Vecchio A, Casolo A, Negro F, et al. The increase in muscle force after 4 weeks of strength training is mediated by adaptations in motor unit recruitment and rate coding. J Physiol. 2019;597(7):1873-1887. https://doi.org/10.1113/JP277250
- Lecce E, et al. Resistance training-induced adaptations in the neuromuscular system: physiological mechanisms and implications for human performance. J Physiol. 2025. https://doi.org/10.1113/JP289716
- Balshaw TG, Massey GJ, Maden-Wilkinson TM, et al. Neural adaptations after 4 years vs 12 weeks of resistance training. Scand J Med Sci Sports. 2019;29(3):348-359. https://doi.org/10.1111/sms.13331
- Skarabot J, Balshaw TG, Maeo S, Folland JP, et al. Contraction intensity-specific effects of training on voluntary activation and agonist EMG amplitude in resistance-trained men. J Appl Physiol. 2021;131(1):189-204. https://doi.org/10.1152/japplphysiol.00148.2021
- Mattocks KT, Buckner SL, Jessee MB, et al. Practicing the Test Produces Strength Equivalent to Higher Volume Training. Med Sci Sports Exerc. 2017;49(9):1945-1954. https://doi.org/10.1249/MSS.0000000000001300
- Taber CB, Vigotsky A, Nuckols G, Haun CT. Exercise-induced myofibrillar hypertrophy is a contributory cause of gains in muscle strength. Sports Med. 2019;49(7):993-997. https://doi.org/10.1007/s40279-019-01107-8
- Barbell Medicine. Low Fatigue Training Guide, 2nd Generation. 2025. Section: Hypertrophy mechanisms. https://www.barbellmedicine.com
- Roberts MD, McCarthy JJ, Hornberger TA, et al. Mechanisms of mechanical overload-induced skeletal muscle hypertrophy: current understanding and future directions. Physiol Rev. 2023;103(4):2679-2757. https://doi.org/10.1152/physrev.00039.2022
- Morton RW, Oikawa SY, Wavell CG, et al. Neither load nor systemic hormones determine resistance training-mediated hypertrophy or strength gains in resistance-trained young men. J Appl Physiol. 2016;121(1):129-138. https://doi.org/10.1152/japplphysiol.00154.2016
- Damas F, Phillips SM, Lixandrao ME, et al. Early resistance training-induced increases in muscle cross-sectional area are concomitant with edema-induced muscle swelling. Eur J Appl Physiol. 2016;116(1):49-56. https://doi.org/10.1007/s00421-015-3243-4
- Damas F, Libardi CA, Ugrinowitsch C. The development of skeletal muscle hypertrophy through resistance training: the role of muscle damage and muscle protein synthesis. Eur J Appl Physiol. 2018;118(3):485-500. https://doi.org/10.1007/s00421-017-3792-9
- DeFreitas JM, Beck TW, Stock MS, et al. An examination of the time course of training-induced skeletal muscle hypertrophy. Eur J Appl Physiol. 2011;111(11):2785-2790. https://doi.org/10.1007/s00421-011-1905-4
- Lazarczuk SL, et al. Mechanical, material and morphological adaptations of healthy lower limb tendons to mechanical loading: a systematic review and meta-analysis. Sports Med. 2022;52(10):2405-2429. https://doi.org/10.1007/s40279-022-01698-9
- Kubo K, et al. Time course of changes in muscle and tendon properties during strength training and detraining. J Strength Cond Res. 2010;24(1):322-331. https://doi.org/10.1519/JSC.0b013e3181c865e2
- Kubo K, et al. Time course of changes in the human Achilles tendon properties and metabolism during training and detraining in vivo. Eur J Appl Physiol. 2012;112(7):2679-2691. https://doi.org/10.1007/s00421-011-2248-x
- Kistler-Fischbacher M, Weeks BK, Beck BR. The effect of exercise intensity on bone in postmenopausal women: systematic review and meta-analysis. Bone. 2021;143:115696. https://doi.org/10.1016/j.bone.2020.115696
- Watson SL, et al. High-intensity resistance and impact training improves bone mineral density in postmenopausal women: the LIFTMOR randomized controlled trial. J Bone Miner Res. 2018;33(2):211-220. https://doi.org/10.1002/jbmr.3284
- Wolff J. Das Gesetz der Transformation der Knochen. Berlin: Hirschwald; 1892.
- Aasa U, et al. Injuries among weightlifters and powerlifters: a systematic review. Br J Sports Med. 2017;51(4):211-219. https://doi.org/10.1136/bjsports-2016-096037
- Keogh JW, Winwood PW. The Epidemiology of Injuries Across the Weight-Training Sports. Sports Med. 2017;47(3):479-501. https://doi.org/10.1007/s40279-016-0575-0
- Prieto-Gonzalez P, et al. Injuries in Novice Participants during an Eight-Week Start up CrossFit Program. Int J Environ Res Public Health. 2020;17(5):1737. https://doi.org/10.3390/ijerph17051737
- Raske A, Norlin R. Injury incidence and prevalence among elite weight and power lifters. Am J Sports Med. 2002;30(2):248-256. https://doi.org/10.1177/03635465020300021701
- Kanayama G, DeLuca J, Meehan WP, et al. Ruptured Tendons in Anabolic-Androgenic Steroid Users: A Cross-Sectional Cohort Study. Am J Sports Med. 2015;43(11):2638-2644. https://doi.org/10.1177/0363546515602010
- Enoka RM, Duchateau J. Translating fatigue to human performance. Med Sci Sports Exerc. 2016;48(11):2228-2238. https://doi.org/10.1249/MSS.0000000000000929
- Behrens M, Gube M, Chaabene H, et al. Fatigue and Human Performance: An Updated Framework. Sports Med. 2023;53:7-31. https://doi.org/10.1007/s40279-022-01748-2
- Meeusen R, Duclos M, Foster C, et al. Prevention, diagnosis, and treatment of the overtraining syndrome: joint consensus statement of the European College of Sport Science and the American College of Sports Medicine. Med Sci Sports Exerc. 2013;45(1):186-205. https://doi.org/10.1249/MSS.0b013e318279a10a
- Halperin I, Emanuel A. Rating of Perceived Effort: Methodological Concerns and Future Directions. Sports Med. 2020;50(4):679-687. https://doi.org/10.1007/s40279-019-01229-z
- Halperin I, Malleron T, Har-Nir I, et al. Accuracy in Predicting Repetitions to Task Failure in Resistance Exercise: A Scoping Review and Exploratory Meta-analysis. Sports Med. 2022;52(2):377-390. https://doi.org/10.1007/s40279-021-01559-x
- Malleron T, Har-Nir I, Vigotsky AD, Halperin I. Effects of imposed versus self-selected upper anchors on perceived effort in resistance training. J Hum Kinet. 2025. https://doi.org/10.5114/jhk/183040
- McHugh MP. Recent advances in the understanding of the repeated bout effect: the protective effect against muscle damage from a single bout of eccentric exercise. Scand J Med Sci Sports. 2003;13(2):88-97. https://doi.org/10.1034/j.1600-0838.2003.02477.x
- Skarabot J, Brownstein CG, Casolo A, Del Vecchio A, Ansdell P. The knowns and unknowns of neural adaptations to resistance training. Eur J Appl Physiol. 2021;121(3):675-685. https://doi.org/10.1007/s00421-020-04567-3
- Garcia-Ramos A, et al. Greater neuromuscular and perceptual fatigue after low-load to failure than heavy-load to failure bench press. J Sports Sci. 2024. https://doi.org/10.1080/02640414.2024.2400798
- Minor B, Helms E, Schepis J. RE: Mesocycle Progression in Hypertrophy: Volume Versus Intensity. Strength Cond J. 2020;42(5):121-124. doi:10.1519/SSC.0000000000000581
- Saw AE, Main LC, Gastin PB. Monitoring the athlete training response: subjective self-reported measures trump commonly used objective measures: a systematic review. Br J Sports Med. 2016;50(5):281-291. https://doi.org/10.1136/bjsports-2015-094758
- Grgic J, Lazinica B, Schoenfeld BJ, Pedisic Z. Test-Retest Reliability of the One-Repetition Maximum Strength Test: a Systematic Review. Sports Med Open. 2020;6(1):31. https://doi.org/10.1186/s40798-020-00260-z
- Zourdos MC, Dolan C, Quiles JM, et al. Efficacy of daily one-repetition maximum training in well-trained powerlifters and weightlifters. Nutricion Hospitalaria. 2016;33(6):1408-1416. https://doi.org/10.20960/nh.806
- Erskine RM, Fletcher G, Folland JP. The contribution of muscle hypertrophy to strength changes following resistance training. Eur J Appl Physiol. 2014;114(6):1239-1249. https://doi.org/10.1007/s00421-014-2855-4
- Maden-Wilkinson TM, Balshaw TG, Massey GJ, Folland JP. What makes long-term resistance-trained individuals so strong? A comparison of skeletal muscle morphology, architecture, and joint mechanics. J Appl Physiol. 2020;128(4):1000-1011. https://doi.org/10.1152/japplphysiol.00224.2019
- Henneman E, Somjen G, Carpenter DO. Functional significance of cell size in spinal motoneurons. J Neurophysiol. 1965;28:560-580.
- Mosso A. La Fatica. Milano: Treves; 1891.
- Morpurgo B. Über Aktivitäts-Hypertrophie der willkürlichen Muskeln. Archiv für Pathologische Anatomie und Physiologie und für klinische Medizin. 1897;150:522-554.
- Schoenfeld BJ, Grgic J, Ogborn D, Krieger JW. Strength and hypertrophy adaptations between low- vs. high-load resistance training. J Strength Cond Res. 2017;31(12):3508-3523. https://doi.org/10.1519/JSC.0000000000002200
- Schoenfeld BJ, Grgic J, Van Every DW, Plotkin DL. Loading recommendations for muscle strength, hypertrophy, and local endurance. Sports Med. 2021;51(6):1073-1095. https://doi.org/10.1007/s40279-021-01490-1
- Barbell Medicine. Training Plateau Action Plan. 2026. https://www.barbellmedicine.com
- Hwang PS, et al. Resistance training-induced elevations in muscular strength in trained men are maintained after 2 weeks of detraining. J Strength Cond Res. 2017;31(4):869-881. https://doi.org/10.1519/JSC.0000000000001807
- Bosquet L, Berryman N, Dupuy O, et al. Effect of training cessation on muscular performance: a meta-analysis. Scand J Med Sci Sports. 2013;23(3):e140-149. https://doi.org/10.1111/sms.12047
- Hakkinen K, Alen M, Komi PV. Changes in isometric force and relaxation time, electromyographic and muscle fibre characteristics during strength training and detraining. Acta Physiol Scand. 1985;125(4):573-585. https://doi.org/10.1111/j.1748-1716.1985.tb07759.x
- Grgic J, Grgic I. Resistance training-induced gains in rate of force development are maintained during detraining. Strength Cond J. 2022. https://doi.org/10.1519/SSC.0000000000000737
- Smith K, Winegard K, Hicks AL, McCartney N. Two years of resistance training in older men and women: the effects of three years of detraining on the retention of dynamic strength. Can J Appl Physiol. 2003;28(3):462-474. https://doi.org/10.1139/h03-035
- Spiering BA, Mujika I, Sharp MA, Foulis SA. Maintaining Physical Performance: The Minimal Dose. J Strength Cond Res. 2021;35(5):1449-1458. https://doi.org/10.1519/JSC.0000000000003964
- Langberg H, Skovgaard D, Petersen LJ, Bülow J, Kjær M. Type I collagen synthesis and degradation in peritendinous tissue after exercise determined by microdialysis in humans. J Physiol. 1999;521(Pt 1):299-306. https://doi.org/10.1111/j.1469-7793.1999.00299.x
- Langberg H, Rosendal L, Kjær M. Training-induced changes in peritendinous type I collagen turnover determined by microdialysis in humans. J Physiol. 2001;534(Pt 1):297-302. https://doi.org/10.1111/j.1469-7793.2001.00297.x
- Lambrianides Y, Epro G, Smith K, Mileva KN, James D, Karamanidis K. Impact of Different Mechanical and Metabolic Stimuli on the Temporal Dynamics of Muscle Strength Adaptation. J Strength Cond Res. 2022;36(11):3246-3255. https://doi.org/10.1519/JSC.0000000000004300
- Latella C, et al. Strength adaptations across the lifespan in competitive powerlifters: a 15-year retrospective and longitudinal growth model. Sports Medicine. 2024. PMID 38060089.
- Ahtiainen JP, Pakarinen A, Alen M, Kraemer WJ, Häkkinen K. Muscle hypertrophy, hormonal adaptations and strength development during strength training in strength-trained and untrained men. Eur J Appl Physiol. 2003;89(6):555-563. https://doi.org/10.1007/s00421-003-0833-3
- Cox J, Chism K, Pritchett L, et al. Efficacy of daily one-repetition maximum bench press training in physically active males and females. Journal of Exercise Physiology Online. 2025;28(1):1-10.
- Bullock N, Hopkins WG. Methods for tracking athletes’ competitive performance in skeleton. J Sports Sci. 2009;27(9):937-940. https://doi.org/10.1080/02640410902763401
- Mendez-Villanueva A, Mujika I, Bishop D. Variability of competitive performance assessment of elite surfboard riders. J Strength Cond Res. 2010;24(1):135-139.
- McGuigan MR, Kane MK. Reliability of performance of elite Olympic weightlifters. J Strength Cond Res. 2004;18(3):650-653.
- Schoenfeld BJ, Ogborn D, Krieger JW. Dose-response relationship between weekly resistance training volume and increases in muscle mass: A systematic review and meta-analysis. J Sports Sci. 2017;35(11):1073-1082.
- Ralston GW, Kilgore L, Wyatt FB, Baker JS. The Effect of Weekly Set Volume on Strength Gain: A Meta-Analysis. Sports Med. 2017;47(12):2585-2601.
- Schoenfeld BJ, Grgic J, Krieger J. How many times per week should a muscle be trained to maximize muscle hypertrophy? A systematic review and meta-analysis of studies examining the effects of resistance training frequency. J Sports Sci. 2019;37(11):1286-1295.
The post Progressive Loading Part 3: The Death of the Novice-Intermediate-Advanced Framework appeared first on Barbell Medicine.